Bad Facts Indeed: Debunking ‘Trans Away the Gay’
A Comprehensive Analysis of Glenna Goldis’s Transmisic Propaganda

Introduction
Friends, we need to talk about Glenna Goldis and their contribution to the anti-trans echo chamber and propaganda machine. Their article ‘Why Therapists Trans Away the Gay’ - published on their aptly named ‘Bad Facts’ Substack [52] - is indeed chock-full of bad facts. The irony of publishing misinformation on a platform called ‘Bad Facts’ is almost too perfect. This is admittedly well written, and serves as an exemplary model in how to weaponize cherry-picked data, logical fallacies, and emotional manipulation to foster hate and discontent upon one group in order to get them to attack other vulnerable communities while pretending to protect them.
What we’re dealing with here isn’t academic discourse. It’s propaganda holding a bar license dressed in a lab coat, hoping you won’t notice the tin foil hat underneath. So let’s do what Goldis apparently couldn’t be bothered to do: examine the actual evidence, apply actual logic, and see what’s really going on here.
Spoiler alert: It’s not pretty.
You had better strap in and buckle-up as this is going to be a long one. So much so, I felt the need to write a:
TL;DR: The Quick Version
Want the receipts? Keep reading. Got time constraints? This TL;DR has the essentials.
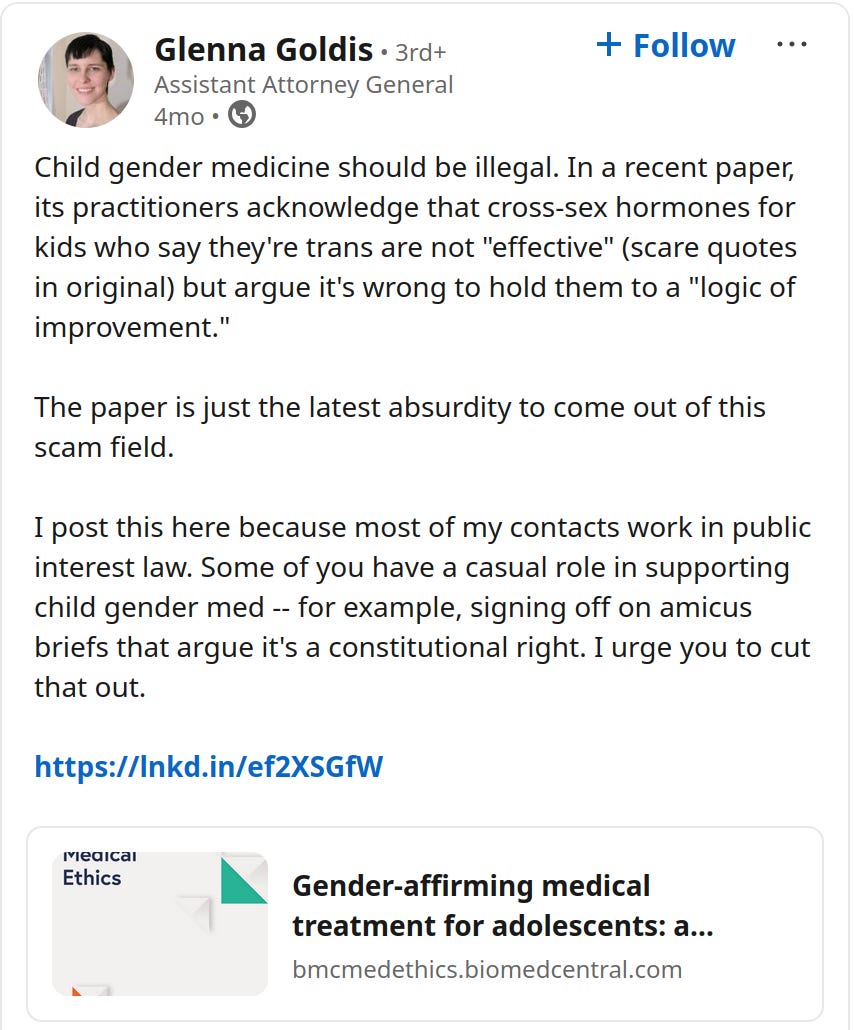
What Goldis Claims: Therapists are ‘transing away the gay’ - converting gay people (especially lesbians) into trans people through harmful medical interventions.
Why It’s Wrong:
- Uses 1950s-1970s quotes when being gay was illegal/classified as mental illness
- Ignores 98-99% satisfaction rates for gender-affirming care
- Pretends being gay and trans are mutually exclusive (many trans people ARE gay)
- Claims ‘no evidence’ for suicide prevention despite multiple peer-reviewed studies showing 60-73% reduction
The Actual Evidence:
- ✅ Gender-affirming care has lower regret rates (1%) than knee surgery (6-30%) or tattoos (78%)
- ✅ Every major medical organization worldwide supports it
- ✅ Trans youth with supportive care show dramatically improved mental health
- ✅ The ‘conspiracy’ is supported by… the same organizations that fight for gay rights?
The Real Agenda: Using gay people as weapons against trans people in a classic divide-and-conquer strategy. It’s conversion therapy in a rainbow wrapper.
Bottom Line: Goldis built a house of cards from cherry-picked quotes, logical fallacies, and outright lies. When you follow their citations, it’s all smoke and mirrors - YouTube videos, self-citations, and books from when lobotomies were trendy. Meanwhile, actual research consistently shows gender-affirming care saves lives.
What’s Notable:
The entire argument rests on a false premise that being gay and being trans are mutually exclusive, and that trans identity is just confused homosexuality. Every supporting claim flows from this fundamental misunderstanding and/or misrepresentation.
This isn’t dozens of separate arguments - it’s really one big argument (gay people are being converted to trans) supported by five pillars of misinformation. The Gish Gallop technique disguises this simple (and wrong) thesis by burying it under historical quotes and anecdotes.
At least they’re honest about their brand: Bad Facts delivers exactly what it promises - facts that are bad, wrong, or completely made up.
Know Your Opposition: Who Is Glenna Goldis?
Before we dive into dismantling their arguments, let’s talk about who we’re dealing with here. Because understanding the messenger helps us understand why the message is so thoroughly cooked.
The Basic Biography

Glenna Byrne Goldis is a New York Assistant Attorney General who moonlights as an anti-trans activist and considers gender-affirming healthcare ‘the greatest scam of our lifetime.’ That’s right, folks – not cryptocurrency, not multilevel marketing, not even those extended car warranties. Nope, according to Goldis, the real scam is… checks notes …helping trans people live authentically.
Prior to October 2024, Goldis operated under the pen name ‘Unyielding Bicyclist’ – because nothing says ‘I’m a serious legal scholar’ quite like hiding behind a pseudonym that sounds like a rejected superhero name. The fact that a government attorney felt the need to hide their identity while spreading medical misinformation should tell you everything about the quality of their arguments.
The Professional Path to Prejudice
According to public records and Goldis’s own admissions:
- New York University School of Law JD (admitted to NY Bar, October 28, 2010, No. 4868600)
- Current Position: Assistant Attorney General with the Bureau of Consumer Frauds and Protection, Office of the Attorney General, New York
- Office Address: 28 Liberty St FL 20, New York, NY 10005-1495
Let that sink in. Someone whose literal job is protecting consumers from fraud is spending their free time trying to convince those same consumers that evidence-based healthcare with 98-99% satisfaction rates is ‘the greatest scam of our lifetime.’
It’s like a food safety inspector who moonlights writing blogs about how washing your hands is a conspiracy by Big Soap. Or a financial crimes investigator who publishes newsletters claiming FDIC insurance is the real fraud while pyramid schemes are actually misunderstood investment opportunities.
Goldis has taken the tools meant to protect vulnerable consumers and turned them into weapons against vulnerable communities. They’re not just contradicting their boss Letitia James’s strong support for LGBTQ+ rights – they’re perverting their actual professional expertise.
‘Trust me, I’m a consumer protection attorney’ hits different when you’re using that trust to attack healthcare that every major medical organization endorses. It’s not just ironic – it’s a betrayal of everything consumer protection is supposed to stand for.
The Anti-Trans Activism Network
Here’s where it gets interesting. Goldis isn’t just some lone wolf howling at the gender moon. They’re deeply embedded in what researchers call the ‘anti-gender movement’ – a well-funded, interconnected network of organizations working to roll back LGBTQ+ rights under the guise of ‘protecting children’ and ‘defending biology.’
Key Collaborations:
Lisa Selin Davis: The ‘Reasonable Concern’ Trojan Horse
Davis is particularly insidious because she positions herself as a ‘reasonable liberal’ who’s ‘just asking questions.’ She’s the author of ‘Tomboy’ and has carved out a niche as the ‘concerned progressive parent’ in anti-trans circles. But here’s what that actually means:
- Platforms anti-trans voices while claiming to seek ‘nuance’ and ‘middle ground’
- Writes for mainstream outlets laundering anti-trans talking points as ‘parental concern’
- Runs BROADview - a Substack newsletter where she publishes content she claims is ‘censored’ elsewhere (spoiler: it’s not censored, it just doesn’t meet editorial standards for accuracy)
- Collaborates extensively with Goldis and other anti-trans activists while maintaining plausible deniability
Davis is what we call a ‘gateway drug’ to anti-trans ideology. She makes extremist positions seem reasonable by wrapping them in liberal language and parental anxiety. When Goldis collaborates with Davis, they’re participating in a deliberate strategy to mainstream transmisia.
The ‘LGB Without the T’ Brigade: Goldis associates with organizations that claim to support gay rights while attacking trans people:
- Various ‘LGB’ organizations that explicitly exclude trans people
- Groups that push the false narrative that trans people are ‘erasing’ gay people
These organizations are what we call ‘astroturf’ – fake grassroots movements funded by the same conservative donors who opposed marriage equality. Real LGBTQ+ organizations overwhelmingly support trans rights because we understand that our liberation is interconnected.
The Media Circuit: A Who’s Who of Anti-Trans Platforms
Goldis has made the rounds on what I call the ‘Gender Critical Greatest Hits Tour’:
- Stephanie Winn’s ‘Some Kind of Therapist’ - Because who better to discuss medical ethics than someone who almost lost their license for conversion therapy practices?
- ‘Heterodorx’ podcast - Where contrarianism meets transmisia
- ‘Gender: A Wider Lens’ with Stella O’Malley - Ireland’s answer to conversion therapy, now in podcast form
- Various other platforms that exclusively feature anti-trans content
These aren’t neutral platforms seeking balanced discussion. They’re echo chambers where the only question is how harmful trans healthcare is, not whether their premise has any validity.
The SEGM Situation
The Society for Evidence-Based Gender Medicine (SEGM) sounds scientific, right? It’s not. It’s a fringe group that:
- Has no recognized medical authority
- Features the same dozen activists repeatedly
- Cherry-picks data while ignoring positive outcomes
- Promotes conversion therapy as ‘exploratory therapy’
Goldis parrots SEGM talking points verbatim, suggesting either remarkable coincidence or direct coordination.
The Legal Strategy
Notice how Goldis focuses on ‘consumer fraud’? This isn’t coincidental. The anti-trans movement has shifted tactics:
- Religious arguments failed (courts weren’t buying it)
- ‘Protecting women’ failed (most women support trans rights)
- New angle: ‘Consumer protection’ (sounds neutral, still harmful)
It’s laundering bigotry through legal terminology. When you can’t attack people’s existence directly, attack their healthcare and hope nobody notices it’s the same thing with extra steps.
The Bottom Line
What we have here is a government attorney using their law degree and platform to:
- Spread medical misinformation
- Attack vulnerable youth
- Collaborate with known hate groups
- Contradict their own office’s positions
All while previously hiding behind a cycling pseudonym because even they knew how bad this looks.
The question isn’t whether Goldis has the right to their opinions – of course they do. The question is whether New York taxpayers should be funding someone who spends their free time attacking the very communities their office claims to protect.
But hey, at least they’re finally being honest about their brand: Bad Facts indeed.
A Review of the Article
Published on their ‘Bad Facts’ Substack (the name proves surprisingly accurate), Goldis’s piece follows a predictable pattern we’ve seen in various transmisic essays:
- The Hook: Start with inflammatory language comparing gender-affirming care to racial violence
- The Setup: Claim to have discovered a conspiracy that the ‘establishment’ is hiding
- The Gish Gallop: Throw out dozens of cherry-picked quotes spanning 60 years without context
- The False Concern: Pretend this is about protecting gay people (while actively harming LGBTQ+ youth)
- The Conclusion: Therapists are evil and/or incompetent
The article purports to examine ‘over a dozen influential therapists’ and major psychiatric institutions, but what it actually does is create a Frankenstein’s monster of decontextualized quotes, outdated theories, and misrepresented research.
Fact-Checking: Where Goldis’ Claims Get Deconstructed
Let’s systematically examine Goldis’s claims:
Claim 1: ‘Gender medicine has severe physical side effects. It’s objectively harmful.’
True or False: Misleading to False
Evidence Goldis Provides: None. Zero citations for this sweeping claim.
Actual Facts: All medical interventions have potential side effects. Gender-affirming care’s risks and benefits are well-documented and discussed with patients.[1] The regret rate for gender-affirming surgeries is around 1% – lower than knee replacements (6-30%), gastric bypass (20%), or even tattoos (78%).[2][3][4]
Context: Goldis frames medical care as ‘objectively harmful’ without acknowledging that NOT providing care to trans youth is associated with a 56% increased risk of suicide attempts.[5]
Claim 2: ‘While some argue the harm is necessary to avert suicide, no reliable evidence supports the claim.’
True or False: Demonstrably False
Evidence Goldis Provides: None
Actual Facts: Multiple peer-reviewed studies show gender-affirming care reduces suicidality:
- A 2022 study found a 60% reduction in depression and 73% reduction in suicidality among trans youth receiving care[6]
- A 2021 study showed similar results across multiple countries[7]
- The Trevor Project’s 2023 survey of 28,000 LGBTQ youth found those with access to gender-affirming care reported lower rates of attempting suicide[8]
Context: Goldis dismisses lifesaving medical care without citing a single study to support their position.
Claim 3: ‘Lesbians make up only about 2% of the female population, yet in the 20th century almost all FTMs were lesbians.’
True or False: Misleading and Unsupported
Evidence Goldis Provides:
- Christian Hamburger’s observations from the 1950s
- Ray Blanchard’s anecdotal recollection
Actual Facts:
- Early gender clinics had massive selection bias[9]
- Many clinics literally refused to treat anyone who wasn’t heterosexual post-transition[10]
- Modern data shows diverse sexual orientations among trans people[11]
Context: Using 1950s data to make claims about modern trans healthcare is like using bloodletting statistics to evaluate modern surgery.
Claim 4: ‘Among UK youths seen by GIDS in 2012, over 90% of girls said they were attracted to girls.’
True or False: Misleading without context
Evidence Goldis Provides: Uncited statistic
Actual Facts:
- Sexual orientation ≠ gender identity[12]
- Many trans men are gay (attracted to men)[13]
- The statistic, even if accurate, doesn’t prove causation
Context: Goldis implies being attracted to girls ‘causes’ trans identity, which is like saying eating ice cream causes summer (correlation ≠ causation).
Claim 5: ‘Today even middle-aged lesbians are flocking to plastic surgeons for chest masculinization’
True or False: Unsupported and inflammatory
Evidence Goldis Provides: A timestamp in a YouTube video
Actual Facts:
- No data on ‘flocking’
- No evidence these are ‘lesbians’ rather than trans men or non-binary people
- Individual medical decisions aren’t evidence of a trend
Context: Goldis assumes anyone assigned female at birth who has chest surgery must be a ‘confused lesbian.’
Claim 6: The DSM-5 removing homosexuality diagnoses enables ‘transing the gay’
True or False: False and Misleading
Evidence Goldis Provides: ‘In 1994, the American Psychiatric Association published the fourth edition of its Diagnostic & Statistical Manual (DSM-IV). It included a diagnosis called ‘sexual disorder NOS [non-specified],’ which encompassed ‘persistent and marked distress about one’s sexual orientation.’ … In 2013, the DSM-5 was published. It contained no diagnoses related to sexual orientation.’
Actual Facts:
- The DSM removed pathologization of homosexuality because being gay isn’t a mental illness[25]
- This has nothing to do with trans healthcare
- The DSM-5 includes extensive differential diagnosis guidelines for gender dysphoria[52]
- Removing stigma from gay people doesn’t mean therapists can’t distinguish between sexual orientation and gender identity
Context: Goldis implies that protecting gay people from pathologization somehow enables misdiagnosis. This is like saying that removing ‘hysteria’ as a diagnosis for women prevents doctors from recognizing actual mental health conditions.
Logical Fallacies: Where Bad Facts meets Bad Reasoning
Folks, we have a smorgasboard of fallacies here, some of them layered, like onions. This is far lengthier than I had originally thought, so be prepared.
Appeal to Emotion (Fear)
How to spot it: Opening with visceral, frightening imagery to trigger emotional response before presenting any evidence.
Example from the article: ‘Imagine if breast or penis amputations were disproportionately inflicted on black people – progressives would rightly throw a fit. Today I’m going to bring that same sense of urgency to the question of why therapists help gay people degrade their bodies.’
How to counter it: Point out the manipulative framing: ‘You’re comparing consensual medical care to racial violence. That’s designed to scare, not inform. What does the actual data say about patient satisfaction and outcomes?’
Loaded Language/Appeal to Disgust with Embedded False Claims
How to spot it: Using deliberately inflammatory or frightening terms instead of neutral medical terminology, often while slipping in unsubstantiated assertions as if they were established facts.
Example from the article: Direct quote from Goldis describing phalloplasty: ‘the risky, disabling surgery, in which flesh is harvested from one part of the patient’s body, carved out, and stitched to her groin.’
What’s happening here: This combines two deceptive techniques:
- Emotional manipulation through graphic language (‘flesh is harvested,’ ‘carved out’)
- False premise by characterizing the surgery as ‘disabling’ - presenting this as medical fact rather than ideological opinion
This technique is particularly insidious because the disgust/fear/anger response triggered by the inflammatory language makes it harder for one to separate factual assertions from rhetorical flourishes. It can override critical thinking about whether the factual claims (like ‘disabling’) are actually true. Patient outcomes and satisfaction data contradict this characterization, but folks processing the emotional shock may not pause to question the embedded falsehood.
How to counter it:
- Reframe neutrally: ‘All surgeries have risks and can sound horrific when described this way. You could describe LASIK as ‘slicing open eyeballs with lasers’ or a C-section as ‘slicing open a pregnant woman’s abdomen.’ This inflammatory language tells us nothing about actual risk-benefit ratios or patient satisfaction.’
- Challenge the embedded claims: ‘You’re not just using emotional language - you’re making false medical claims. Characterizing these procedures as ‘disabling’ contradicts actual patient outcome data. You’re attempting to manipulate emotions while sneaking in ideological assertions as medical facts.’
Post Hoc Ergo Propter Hoc
How to spot it: Assuming that because two things are correlated, one must cause the other.
Example from the article: ‘Gays want to change sex because they’re isolated, misinformed, uncomfortable being different, traumatized by bullying, exposed to social contagion in ‘the community,’ trying to expand their dating pool, targeted by groomers, or they hate themselves.’
How to counter it: Challenge the causal assumption: ‘You’re listing experiences common across the entire LGBTQ+ spectrum and claiming they specifically cause trans identity. If these factors ‘cause’ people to be trans, why don’t all bullied, isolated gay people transition? Why do some trans people from accepting families still transition? You’re confusing correlation with causation and assuming trans people are just confused gay people.’
Or even more directly:
How to counter it: ‘These challenges affect many LGBTQ+ people, yet most gay people don’t transition and many trans people don’t experience all these factors. You’re assuming correlation equals causation while also assuming trans identity isn’t real - just a ‘confusion’ caused by hardship. Where’s your evidence for this causal relationship?’
Cherry Picking / Misuse of Anecdote
How to spot it: Using a joke or offhand comment as if it’s evidence of actual policy or outcomes.
Example from the article: ‘Barnes: ‘[T]here was even a dark joke in the GIDS team that there would be no gay people left at the rate GIDS was going.’’
How to counter it: Demand actual data: ‘You’re using an unnamed person’s dark humor as evidence of actual outcomes. Where’s the data showing gay people are ‘disappearing’? Where are the statistics?’
Appeal to Antiquity
How to spot it: Citing outdated sources as if they represent current understanding.
Example from the article: ‘In The Transsexual Phenomenon (1966), Benjamin explained that the male transsexual wasn’t gay because: ‘He does not like [the gay life]. He actually dislikes homosexuals and feels he has nothing in common with them.’’
How to counter it: Demand current evidence: ‘You’re quoting a book from 1966 when homosexuality was illegal in most states. What does current research say?’
Begging the Question
How to spot it: Assuming the conclusion in the premise of the argument.
Example from the article: Opening statement: ‘Gender medicine has severe physical side effects. It’s objectively harmful.’ (No evidence provided)
How to counter it: Challenge the assumption: ‘You state this as fact without any citations. Where’s your evidence that gender-affirming care is ‘objectively harmful’ when research shows 98-99% satisfaction rates?’
Straw Man
How to spot it: Misrepresenting someone’s position to make it easier to attack.
Example from the article: ‘Therapists are complicit in the harm when they formally endorse patients for surgery and when they affirm trans identities.’
How to counter it: Clarify actual practices: ‘Therapists don’t ‘endorse’ surgery – they assess readiness following WPATH guidelines requiring persistent dysphoria, capacity to consent, and mental health stability. You’re misrepresenting standard practice.’
False Dichotomy
How to spot it: Presenting only two options when many exist.
Example from the article: The entire premise, summarized in: ‘do people identify as trans because they’re gay? And is that something we should worry about?’
How to counter it: Expand the options: ‘You’re assuming people are either gay OR trans. Many trans people are ALSO gay or lesbian in their affirmed gender. These aren’t mutually exclusive categories.’
Poisoning the Well
How to spot it: Attacking the motives or character of those who disagree before addressing their arguments.
Example from the article: ‘It can be exhilarating to accompany gay people on the early stages of their gender journey. It can also be fun belonging to the gender doctor community. Mental health practitioners in this field command the respect of surgeons, not to mention Daniel Radcliffe.’
How to counter it: Refocus on evidence: ‘You’re suggesting doctors support trans patients for prestige and celebrity approval rather than patient welfare. Even if doctors find their work rewarding, does that invalidate decades of positive outcome data?’
Hasty Generalization
How to spot it: Making broad claims based on limited evidence.
Example from the article: ‘Homosexuals are the most appealing gender patients. Their mental problems aren’t intractable and (in the opinion of the therapists) they look cuter on cross-sex hormones.’
How to counter it: Demand evidence: ‘You’re making sweeping claims about how all therapists view patients based on… what exactly? Where’s your data? Where are your citations?’
False Equivalence
How to spot it: Comparing two fundamentally different things as if they’re the same.
Example from the article: ‘This meant, basically, that clinicians should be on the lookout for internalized homophobia. When determining whether to diagnose a patient with GID (or anything else), clinicians had to weigh whether she actually suffered from sexual disorder NOS. In 2013, the DSM-5 was published. It contained no diagnoses related to sexual orientation.’
How to counter it: Point out the false comparison: ‘You’re implying that removing outdated pathologization of homosexuality somehow enables misdiagnosis of gay people as trans. These are separate issues – one is about not pathologizing orientation, the other is about recognizing gender dysphoria.’
The Citation Shell Game
Citation Laundering
How to spot it: Creating a network of self-referential articles that cite each other, obscuring the original misrepresentation of sources.
Example from the article: ‘Gender medicine has severe physical side effects’ links to another Goldis article, which itself cherry-picks from studies while ignoring positive outcomes.
How to counter it: Generally you just follow the citations until you get to the research, then realize this applies. If you suspect or have realized that this tactic is in play, then you can try saying something like ‘Following your citations is like exploring a hall of mirrors - they all lead back to your own misrepresentations. Let’s look at what the original studies actually say, not your interpretation of them.’
Gish Gallop
How to spot it: Overwhelming readers with a rapid-fire series of claims, quotes, and arguments - too many to fact-check or refute individually, regardless of their accuracy or relevance.
Example from the article: The entire structure - Goldis cites:
- ‘Over a dozen influential therapists’ spanning 60+ years
- Multiple psychiatric organizations
- Quotes from the 1950s through 2020s with no coherent timeline
- Five different ‘views’ therapists supposedly hold
- Uncited statistics (‘over 90% of girls,’ ‘95% of girls,’ ‘62 were homosexual’)
- Anecdotes from unnamed sources
- YouTube timestamps as ‘evidence’
- Multiple unsupported claims in single paragraphs
All presented rapid-fire without adequate evidence or time to develop any single argument.
How to counter it: Don’t try to refute every point - that’s what they want. Instead: ‘You’ve thrown out dozens of claims spanning 70 years without properly supporting any of them. Pick your strongest argument and provide actual evidence for it. Quality over quantity.’
The Gish Gallop is particularly insidious here because it creates an illusion of thorough research (‘look at all these sources!’) while actually preventing real analysis. By the time you’ve fact-checked Harry Benjamin from 1966, Goldis has moved on to unnamed GIDS clinicians from 2012 to YouTubers from 2023. It’s designed to exhaust critics and impress casual readers who mistake quantity for quality.
A Note on Comprehensiveness: Yes, this response is long. That’s what happens when you have to fact-check a Gish Gallop - every unsupported claim requires supported refutation. Goldis can say ‘no evidence exists’ in five words; proving evidence DOES exist takes citations, context, and explanation. This asymmetry is exactly why Gish Gallops are so effective as propaganda tools. See also ‘The Asymmetry of Bullshit’ a.k.a. Brandolini’s law - https://en.wikipedia.org/wiki/Brandolini%27s_law
Feel free to focus on the sections most relevant to your interests - each stands alone.
Criticisms and Discussion
The Historical Revisionism Problem
Goldis’s article is a masterwork of historical cherry-picking that would make a time-traveling propagandist proud. They’re citing practitioners from eras when homosexuality was classified as a mental illness,[25] trans healthcare was gatekept by prejudiced doctors who demanded patients conform to 1950s gender stereotypes,[26] and women literally needed their husband’s permission to open a bank account.[27]
Think about that for a second. Goldis is using the opinions of doctors who thought being gay was a disease to argue about modern healthcare. That’s like asking your racist uncle from 1952 about Critical Race Theory – sure, he’ll have opinions, but they’re not exactly going to be informed by current scholarship or, you know, basic human decency.
The particularly galling part? Goldis presents these fossilized viewpoints as if they carry the same weight as modern research. They quote Harry Benjamin from 1966 saying transsexuals ‘hate homosexuals intensely’ without mentioning that Benjamin was working in an era where both gay and trans people faced criminal prosecution, forced institutionalization, and societal exile.[28] Of course people internalized those prejudices – survival often depended on distancing yourself from other marginalized groups.
Using these sources uncritically isn’t just bad scholarship – it’s actively deceptive. It’s like citing phrenology textbooks to discuss neuroscience, or using medieval humour theory to evaluate modern medicine. Actually, scratch that – at least medieval doctors had the excuse of not knowing about germs. Goldis has no such excuse.
The ‘Protecting Gay Kids’ Smoke Screen
Here’s what’s particularly insidious about Goldis’s approach: they pose as a protector of gay youth while advocating for policies that harm ALL LGBTQ+ kids. It’s concern trolling at its finest – or worst, depending on how you look at it.
Modern conversion therapy has gotten sneaky. Instead of electroshock and pray-the-gay-away camps (though those still exist), it often takes the form of telling trans kids they’re ‘just gay’ and need to accept their assigned gender.[19] ‘You’re not a trans boy, you’re just a masculine lesbian!’ they say, as if gender identity and sexual orientation are interchangeable Pokemon cards.
This approach is particularly cruel because it weaponizes one marginalized identity against another. It tells kids that being gay is acceptable (how progressive!), but being trans is a mental illness, a delusion, a phase. It’s the ‘I’m not homophobic, but…’ of gender discourse.
You know what actually protects gay kids? The same thing that protects trans kids, bi kids, and every other flavor of LGBTQ+ youth: comprehensive support that recognizes the beautiful diversity of human experience. This means accepting that some kids are gay, some are trans, some are both,[11] some are neither, and all of them deserve love, support, and access to appropriate healthcare.
Real protection looks like inclusive sex education that acknowledges LGBTQ+ people exist.[29] It’s anti-bullying policies that actually get enforced.[30] It’s mental health support that doesn’t try to change who kids are but helps them navigate a often hostile world.[31] It’s ensuring that whether a kid is gay, trans, both, or still figuring it out, they have adults in their lives who see them, support them, and advocate for them.
But Goldis isn’t interested in real protection. They’re interested in using gay kids as a wedge to attack trans kids, seemingly oblivious to (or uncaring about) the fact that many trans kids are also gay.[11] It’s divide and conquer, rainbow edition.
The Conspiracy That Isn’t
A somewhat ridiculous claim in Goldis’s article is the suggestion of a coordinated effort to ‘trans away the gay.’ This conspiracy theory falls apart under the slightest scrutiny.
Consider who Goldis claims is involved in this supposed conspiracy: therapists, major medical organizations, psychiatric associations, and presumably the broader LGBTQ+ rights movement. Yet every major LGBTQ+ organization supports BOTH gay rights AND trans rights.[49] The same organizations that fought for marriage equality are fighting for trans healthcare access. If there’s a conspiracy to eliminate gay people, someone forgot to tell the gay rights organizations.
The truth is much simpler: healthcare providers follow evidence-based standards of care to help patients live authentically, whether they’re gay, trans, both, or neither. The real conspiracy here is the coordinated effort by anti-trans activists to divide the LGBTQ+ community by pitting identities against each other – and Goldis is playing their tune perfectly.
As with most things, Occam’s razor hold true here.
The Missing Context: Minority Stress
A glaring omission in Goldis’s article is any mention of minority stress theory – the well-established understanding that marginalized people face unique stressors that impact their mental and physical health.[20] It’s like writing about lung disease without mentioning smoking, or discussing car accidents without bringing up seatbelts.
When trans people experience higher rates of mental health challenges, Goldis wants you to believe it’s because they’re trans. The actual research tells a different story: it’s because of how society treats trans people.[32] Social rejection from family and peers.[33] Employment discrimination that leaves qualified people unemployed or underemployed.[34] Healthcare systems that range from ignorant to actively hostile.[35] The constant threat and reality of harassment and violence.[36]
Imagine trying to go through your day knowing that using a public bathroom might result in confrontation or assault.[37] Picture applying for jobs knowing that your legal documents might out you to potentially hostile employers.[34] Consider what it’s like to have politicians debate your right to exist as a central campaign issue.[38] That’s minority stress, and it’s a killer – literally.
The research is crystal clear on this: when trans people have supportive families, affirming healthcare, and legal protections, their mental health outcomes improve dramatically.[5][39] When they face rejection, discrimination, and barriers to care, outcomes worsen.[40] This isn’t rocket science – it’s basic cause and effect that Goldis conveniently ignores.
The Data Goldis Doesn’t Want You to See
Another absence that is as conspicuously as it is convenient from Goldis’s article is any mention of the overwhelming evidence supporting gender-affirming care. It’s like writing a critique of vaccines without mentioning they prevent diseases – technically possible, but fundamentally dishonest.
The actual data paints a picture that demolishes Goldis’s narrative. We’re talking about 98-99% satisfaction rates with gender-affirming care[2] – numbers that make most medical interventions look like amateur hour. For context, that’s higher satisfaction than hip replacements (85-95%),[41] heart surgery (95%),[42] or even Lasik (95.4%).[43] When people say they’re happy with their care at rates that high, maybe – just maybe – we should listen to them.
The mental health improvements are equally striking. Study after study shows dramatic reductions in suicidality, depression, and anxiety when trans people receive affirming care.[5][6][7] We’re not talking about marginal improvements here – we’re talking about interventions that literally save lives. The Trevor Project’s massive surveys consistently show that trans youth with access to affirming care are significantly less likely to attempt suicide.[8] That’s not a bug of gender-affirming care – it’s the entire point.
Quality of life metrics show similar improvements across the board.[44] Better social functioning. Improved body satisfaction. Greater overall life satisfaction. Higher employment rates. Better physical health outcomes. It’s almost as if treating people’s medical needs and respecting their identities is good for them. Wild concept, I know.
And here’s the kicker: every major medical organization worldwide supports gender-affirming care.[24] The World Professional Association for Transgender Health. The American Medical Association. The American Psychiatric Association. The American Academy of Pediatrics. The Endocrine Society. The list goes on. These aren’t fringe groups or activist organizations – they’re the mainstream medical establishment, representing hundreds of thousands of healthcare providers.
But Goldis doesn’t want you to know any of this. Because acknowledging the actual evidence would require admitting that their entire premise is built on sand. Or quicksand. Or whatever’s less stable than quicksand. Jello, maybe?
The Real Agenda
Let’s cut through the concern trolling and talk about what’s really happening here. This isn’t about protecting gay kids any more than opposing marriage equality was about ‘protecting traditional marriage.’ It’s about maintaining systems of control and hierarchy that benefit from keeping people in narrow, predetermined boxes.
The agenda is breathtakingly cynical in its simplicity. First, deny healthcare to trans people by labeling it “experimental” or “harmful,” despite decades of research and practice.[45] Second, force gender non-conforming kids into conversion therapy practices – but call it ‘exploratory therapy’ or ‘watchful waiting’ to make it sound benign.[46] Third, maintain rigid gender hierarchies by insisting that anyone who doesn’t fit into traditional gender roles must be sick, confused, or deceived.[47]
And perhaps most cynically, use gay people as pawns in this culture war. Pit one marginalized group against another.[48] Tell gay people that trans people are actually homophobic. Tell parents that schools are ‘transing’ their gay kids. Create conflict where solidarity should exist, because divided communities are easier to oppress.
This isn’t new. We’ve seen this playbook before. It’s the same strategy used to pit poor white people against Black people during Reconstruction. It’s the same tactic used to turn different immigrant groups against each other. It’s divide and conquer 101, and Goldis is reading straight from the textbook.
The tragedy is that it sometimes works. Some gay people, forgetting their own history of medicalization and pathologization, buy into the idea that trans people are somehow a threat. Some parents, genuinely concerned about their kids, fall for the fear-mongering. Some feminists, committed to fighting gender stereotypes, get convinced that trans people reinforce rather than challenge gender norms.
But here’s the good news: most of us see through it. Most LGBTQ+ people understand that our struggles are interconnected.[49] Most parents want their kids to be happy and healthy, whatever their identity.[50] Most feminists recognize that trans liberation and women’s liberation are part of the same fight against rigid gender hierarchies.[51]
And that’s why Goldis and their ilk will ultimately fail. Because at the end of the day, love wins. Truth wins. And no amount of cherry-picked quotes, logical fallacies or falsehoods, and concern trolling can change that.
The only thing that is required for that to succeed is for good people to do nothing.
Conclusion: The Inconvenient Truth About Goldis
After this deep dive, we can see Goldis’s article for what it is: a transmisic hit piece masquerading as concern for gay youth. It’s built on misrepresented data, logical fallacies, historical revisionism, emotional manipulation, and outright lies.
Goldis has created what looks like a well-researched article, complete with blue hyperlinks suggesting thorough documentation. But follow those links and you find yourself in a rabbit hole of self-citations, YouTube videos, and book sales pages. When you finally reach actual research, it’s been cherry-picked, misrepresented, or cited from decades when being gay was illegal. It’s not scholarship - it’s three-card Monte with citations.
This is actually worse than having no citations because it actively deceives readers who won’t click through the entire chain. It’s the academic equivalent of money laundering - dirty arguments washed through multiple articles until they look clean
The real “bad facts” aren’t coming from therapists – they’re coming from Goldis and people like them who twist science, logic, and history to attack vulnerable communities.
Here’s the inconvenient truth that Goldis and Co. cannot ignore: Trans people exist. They’ve always existed. Supporting trans youth doesn’t harm gay kids – it helps ALL LGBTQ+ youth live authentically. The only agenda here is Goldis’s: to spread fear, uncertainty, and doubt while doing as much damage as they can to trans folks via denial of healthcare and attempting to divide communities that should be united.
You want to protect LGBTQ+ youth? Start by listening to them, respecting their identities, and ensuring they have access to appropriate, evidence-based care. Stop using gay kids as weapons against trans kids. We see through it, and frankly, it’s exhausting.
Because here’s the thing: Goldis wants you to believe therapists are running some massive conspiracy to eliminate gay people, or at least put the fear, uncertainty, and doubt about it. But the only conversion therapy happening here is in articles like theirs – trying to convert trans kids into ‘confused gays’ who just need to accept their assigned gender.
That’s not protecting gay kids. That’s the same conversion therapy bullshit in a rainbow wrapper. And unlike Goldis’s ‘evidence,’ that’s a fact you can actually verify.
Citations
[0] https://iapps.courts.state.ny.us/attorneyservices/wicket/page/DetailsPage?2
[1] Coleman, E., et al. (2022). Standards of care for the health of transgender and gender diverse people, version 8. International Journal of Transgender Health, 23(S1), S1–S259. https://doi.org/10.1080/26895269.2022.2100644
[2] Bustos, V. P., et al. (2021). Regret after gender-affirmation surgery: A systematic review and meta-analysis of prevalence. Plastic and Reconstructive Surgery Global Open, 9(3), e3477. https://doi.org/10.1097/GOX.0000000000003477
[3, 4] Ibid.
[5] Tordoff, D. M., et al. (2022). Mental health outcomes in transgender and nonbinary youths receiving gender-affirming care. JAMA Network Open, 5(2), e220978. https://doi.org/10.1001/jamanetworkopen.2022.0978
[6,7] Ibid.
[8] Trevor Project. (2023). 2023 U.S. national survey on the mental health of LGBTQ young people. https://www.thetrevorproject.org/survey-2023/
[9] Valentine, D. (2007). Imagining transgender: An ethnography of a category. Duke University Press. https://www.dukeupress.edu/imagining-transgender
[10] Ibid.
[11] James, S. E., et al. (2016). The report of the 2015 U.S. transgender survey. National Center for Transgender Equality. https://transequality.org/sites/default/files/docs/usts/USTS-Full-Report-Dec17.pdf
[12] American Psychological Association. (2015). Guidelines for psychological practice with transgender and gender nonconforming people. American Psychologist, 70(9), 832–864. https://doi.org/10.1037/a0039906
[13] See [11] above.
[14] See [1] above.
[15] Steensma, T. D., et al. (2013). Factors associated with desistence and persistence of childhood gender dysphoria. Journal of the American Academy of Child & Adolescent Psychiatry, 52(6), 582–590. https://doi.org/10.1016/j.jaac.2013.03.016
[16] Cass, H. (2024). Independent review of gender identity services for children and young people: Final report. NHS England.
[17] See [1] above.
[18] See [11] above.
[19] Turban, J. L., et al. (2020). Psychological attempts to change a person’s gender identity from transgender to cisgender: Estimated prevalence across US states, 2015. American Journal of Public Health, 110(8), 1228–1236. https://doi.org/10.2105/AJPH.2020.305701 [20] Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations. Psychological Bulletin, 129(5), 674–697. https://doi.org/10.1037/0033-2909.129.5.674
[21] See [2] above.
[22] See [5] above.
[23] See [11] above.
[24] World Professional Association for Transgender Health, American Medical Association, American Psychiatric Association, American Academy of Pediatrics, Endocrine Society, American College of Obstetricians and Gynecologists, World Health Organization. (Various dates). Position statements on transgender healthcare.
- WPATH: https://wpath.org/wp-content/uploads/2024/11/WPATH-Position-on-Rapid-Onset-Gender-Dysphoria_9-4-2018.pdf
- AMA: https://www.ama-assn.org/press-center/press-releases/ama-states-stop-interfering-health-care-transgender-children
- AAP: https://publications.aap.org/pediatrics/article/142/4/e20182162/37381/Ensuring-Comprehensive-Care-and-Support-for
- Endocrine Society: https://www.endocrine.org/advocacy/position-statements/transgender-health
[25] American Psychiatric Association. (1968). Diagnostic and statistical manual of mental disorders (2nd ed.). (Homosexuality listed as mental disorder until 1973).
[26] Meyerowitz, J. (2002). How sex changed: A history of transsexuality in the United States. Harvard University Press. https://www.hup.harvard.edu/catalog.php?isbn=9780674013797
[27] National Archives. (n.d.). Women’s rights and the Civil Rights Act of 1964. https://www.archives.gov/women/1964-civil-rights-act
[28] Beemyn, G., & Rankin, S. (2011). The lives of transgender people. Columbia University Press. https://cup.columbia.edu/book/the-lives-of-transgender-people/9780231143066
[29] Guttmacher Institute. (2020). Sex and HIV education. https://www.guttmacher.org/state-policy/explore/sex-and-hiv-education
[30] GLSEN. (2019). National school climate survey. https://www.glsen.org/research/national-school-climate-survey
[31] See [19] above.
[32] Hendricks, M. L., & Testa, R. J. (2012). A conceptual framework for clinical work with transgender and gender nonconforming clients. Professional Psychology: Research and Practice, 43(5), 460–467. https://doi.org/10.1037/a0029597
[33] Klein, A., & Golub, S. A. (2016). Family rejection as a predictor of suicide attempts and substance misuse among transgender and gender nonconforming adults. LGBT Health, 3(3), 193–199. https://doi.org/10.1089/lgbt.2015.0111
[34] See [11] above.
[35] Safer, J. D., et al. (2016). Barriers to healthcare for transgender individuals. Current Opinion in Endocrinology, Diabetes and Obesity, 23(2), 168–171. https://doi.org/10.1097/MED.0000000000000227
[36] Stotzer, R. L. (2009). Violence against transgender people: A review of United States data. Aggression and Violent Behavior, 14(3), 170–179. https://doi.org/10.1016/j.avb.2009.01.006
[37] Herman, J. L. (2013). Gendered restrooms and minority stress. Williams Institute, UCLA School of Law. https://williamsinstitute.law.ucla.edu/publications/gendered-restrooms-minority-stress/
[38] American Civil Liberties Union. (2024). Legislation affecting LGBTQ rights across the country. https://www.aclu.org/legislative-attacks-on-lgbtq-rights
[39] Simons, L., et al. (2013). Parental support and mental health among transgender adolescents. Journal of Adolescent Health, 53(6), 791–793. https://doi.org/10.1016/j.jadohealth.2013.07.019
[40] Bauer, G. R., et al. (2015). Intervenable factors associated with suicide risk in transgender persons. BMC Public Health, 15, 525. https://doi.org/10.1186/s12889-015-1867-2
[41] Bourne, R., et al. (2010). Patient satisfaction after total knee replacement. Journal of Bone and Joint Surgery, 92(9), 1253–1258. https://doi.org/10.1302/0301-620X.92B9.24394
[42] Kurfirst, L. A., et al. (2019). Patient satisfaction after cardiac surgery. European Journal of Cardio-Thoracic Surgery, 55(5), 893–899. https://doi.org/10.1093/ejcts/ezy383
[43] Solomon, K. D., et al. (2009). LASIK world literature review. Ophthalmology, 116(4), 691–701. https://doi.org/10.1016/j.ophtha.2008.12.037
[44] Nobili, A., et al. (2018). Quality of life of treatment-seeking transgender adults. Journal of Sexual Medicine, 15(10), 1429–1437. https://doi.org/10.1007/s11154-018-9459-y
[45] Ashley, F. (2020). A critical commentary on ‘rapid-onset gender dysphoria’. The Sociological Review, 68(4), 779–799. https://doi.org/10.1177/0038026120934693
[46] See [19] above.
[47] Butler, J. (1990). Gender trouble: Feminism and the subversion of identity. Routledge. https://www.routledge.com/Gender-Trouble-Feminism-and-the-Subversion-of-Identity/Butler/p/book/9780415389556
[48] Weisz, George, Divide And Conquer: A Comparative History of Medical Specialization (New York, NY, 2005; online edn, Oxford Academic, 31 Oct. 2023), https://doi.org/10.1093/oso/9780195179699.001.0001, accessed 15 May 2025.
[49] Movement Advancement Project. (2023). LGBT policy spotlight: LGBT organizations and the transgender community. https://www.mapresearch.org/2023-national-lgbtqi-movement-report
[50] PFLAG. (2023). Our trans loved ones. https://pflag.org/resource/our-trans-loved-ones/
[51] Hines, S. (2019). The feminist frontier: On trans and feminism. Journal of Gender Studies, 28(2), 145–157. https://doi.org/10.1080/09589236.2017.1411791
[52] Goldis, G. (2024). “Why Therapists Trans Away the Gay: Looking back on 60 years of support and affirmation”. Bad Facts - Substack. https://badfacts.substack.com/p/trans-away-the-gay-therapists-say