The Inconvenient Truth About Arty Morty's Transphobic Propaganda
A Point-by-Point Debunking of Arty Morty's Anti-Trans Nonsense
Introduction
Well howdy there PITT crew it's me again, and today we are going to thoroughly debunk the dangerous misconceptions and junk science found in a recent article titled "There are no trans kids, only kids confused about sex" by Arty Morty. Arty, a self-proclaimed “expert” on gender identity, makes a number of alarming claims about trans youth that not only contradict scientific consensus, but echo the usual and insidious myths and talking points of anti-trans activists.
Morty’s article is essentially a manifesto that compiles nearly all the major anti-trans arguments and talking points into a single document. While it's presented in an ostensibly rational and analytical style, it relies heavily on a number of controversial claims and assumptions to make its case, such as:
- Biological sex is the only valid way to categorize people, and gender identity is a delusion
- Being transgender is caused by sexual fetishes in men and internalized homophobia in women
- Medical transition, especially for minors, is unnecessary, harmful, and abusive
- The transgender rights movement is a dangerous quasi-religious cult forcing its ideology on society
- Liberal institutions have been duped or bullied into enabling this harmful transgender agenda
Many of Morty's key assertions - like autogynephilia theory, rapid onset gender dysphoria, and equating transition with mutilation - are heavily disputed by major medical organizations and LGBTQ advocacy groups. The entire piece reflects a particular anti-trans/TERF ideological bias against accepting transgender identities, rights and healthcare as valid.
In fact, we can replace the word “transgender” with “homosexuality”, and “sex” with “gender”, and get the complete anti-gay playbook resurrected and revised, coupled with all the right wing talking points against gay marriage - including all the groomer fear mongering and “it’s popular/trendy to be gay” talking points from bygone years before.
Morty argues that being transgender is a “delusional ideology” rather than a valid identity, that gender-affirming care is a form of “child abuse”, and that the "transgender craze" will inevitably collapse like the lobotomy scandal. I wonder if Kat Highsmith borrowed this from Arty Morty, or if Arty Morty lifted this from Kat Highsmith. In that same vein, these claims are not only factually wrong, but incredibly harmful, and they demand a thorough, evidence-based, point-by-point debunking.
So that is what we are going to do. Far from an objective analysis, Morty's piece relies on unsupported assertions, misrepresentations of research, and some deeply flawed reasoning to push a false narrative about trans youth. Their arguments reflect the same kind of pseudoscience and conspiracy thinking that have long been used to undermine the rights and humanity of marginalized groups.
By denying the reality of trans identities, painting gender-affirming care as reckless experimentation, and comparing the transgender rights movement to a medical scandal, Morty is perpetuating dangerous misconceptions that have real-world consequences. This rhetoric fuels the stigma, discrimination, and barriers to care that trans people already face. With rising rates of anti-trans legislation and violence, it has never been more important to challenge this misinformation.
So in this article, we will systematically dismantle Morty's claims and the fallacies underpinning them. We'll examine the extensive scientific evidence that gender identity has biological roots and that supporting trans youth leads to better mental health outcomes. We'll debunk the myth that being transgender is a mental illness or that gender-affirming care is child abuse. We'll expose the fearmongering and junk science behind Morty's assertions about social contagion and their comparison to medical scandals. And we'll reaffirm the validity of trans identities and the importance of trans-inclusive policies and practices.
Ultimately, this point-by-point takedown will show unequivocally that Morty's article is rooted not in facts but in fear, not in science or data, but in prejudice and confirmation bias. In a time of escalating anti-trans backlash, we must respond to propaganda like this with evidence, compassion and a commitment to the truth. The health and humanity of transgender people depend on it.
So let's dive into dismantling the false claims in "There are no trans kids" - and in doing so, stand up for science, justice and the fundamental rights of all young people to live authentically. Seeing as how this is the first time I have ever heard of or have written about Arty Morty, let’s start with an introduction.
Who is Arty Morty?
Arty Morty is the pseudonym of a Canadian writer and anti-transgender activist who frequently argues against the validity of transgender identities and rights. Morty is probably best known as a sidekick to anti-trans extremist Graham Linehan and, a writer and commentator who frequently shares views on gender identity, transgender activism, and related social and political issues on Substack, YouTube, and as a co-founder of LGB Alliance Canada.12
In Arty's own words, their primary qualifications are being "a humanist and a scientific realist" who views "gender identity ideology as antithetical to my core values." Arty expresses "respect and compassion for transsexuals" while believing that "humans do not change sex" and that gender identity is a harmful concept. 3
However, Arty does not claim any specific professional expertise in fields like psychology, biology, or gender studies, nor mention any relevant academic credentials or research background. Arty's perspectives seem to be based on personal experiences, such as growing up as a "feminine boy" and later identifying as a gay man, and observations of social and political dynamics around gender.4
On YouTube, podcasts, and the Substack blog, Morty expresses an ideological commitment to opposing what is termed "gender identity ideology." 3 Morty has appeared with other activists who argue against social and medical support for transgender people, including youth, such as Sasha Ayad and Stella O'Malley. 4 Some LGBTQ advocates have characterized Morty as an "anti-trans extremist." 5
This background is essential context for readers evaluating the arguments Morty makes about trans youth in the article "There are no trans kids, only kids confused about sex." Morty's close association with Graham Linehan, who has been called a "radicalized extremist transphobe" by Morty himself6, and reputation as an anti-trans extremist in some corners all suggest the article's claims should be approached critically and checked rigorously against scientific evidence. While Morty's perspectives may be sincerely held, they are shaped by an activist agenda that seems to reject the legitimacy of trans identities entirely.
So while Arty presents forceful opinions on trans issues with an authoritative tone7, the lack of cited qualifications or evidence raises questions about the reliability of those views. Arty has a clear ideological agenda, made evident by co-founding LGB Alliance Canada and comparing trans activists to "a dangerous cult" like Scientology.8
Now that we are more familiar with Morty, we can place their lengthy article into the proper context and perspective from which it was written. With that in mind, let’s give the main points of their article a closer look.
Debunking the Main Points
Arty Morty makes three core arguments against the validity of transgender identities and gender-affirming care for youth. First, Morty asserts that being transgender is a "delusional ideology" that defies biological reality. Second, Morty portrays gender-affirming medical care as "child abuse" and "reckless experimentation" on youth. Finally, Morty compares the growing visibility of trans identities to "social contagions" and "crazes" like lobotomies, suggesting it will inevitably collapse. However, all of these claims are contradicted by scientific evidence, expert consensus, and historical records. Let’s break them down together, shall we?
1. The false dichotomy of "natural kinds" vs "non-natural kinds"
The article's first argument rests on a flawed and overly simplistic categorization of gender identity as either a "natural kind" - an immutable, biologically determined trait - or a "non-natural kind" - a socially constructed, chosen identity. Morty contends that because gender identity does not meet their narrow criteria for a "natural kind," it must therefore be an incoherent concept with no basis in reality.
However, this black-and-white view fails to capture the complex interplay of biological, psychological and social factors that actually shape the development of gender identity. As Mazzuca, et al; states:
The Mazzuca et al. study directly challenges Morty's oversimplified "natural kinds" framework by demonstrating that gender emerges from a complex interaction of biological, psychological, and social factors. Through detailed analysis of gender concept formation, the researchers found that specific life experiences shape how people understand and experience gender - it is neither purely biological nor purely social, but rather develops through dynamic interactions between physical embodiment, psychological development, and cultural context. This empirical evidence contradicts Morty's rigid binary categorization and shows that gender identity formation involves multiple interacting dimensions that cannot be reduced to simple either/or categories.
Furthermore, Morty’s assertion that gender identity has no biological basis is contradicted by a growing body of scientific evidence. Numerous brain imaging studies have found that the brain structures of transgender individuals more closely resemble their identified gender than their sex assigned at birth.10 These neuroimaging studies have identified consistent patterns in brain structure and function that align more closely with gender identity than assigned sex at birth. For example, research has found differences in brain regions related to body perception, self-referential thinking, and sexual response that correspond to gender identity rather than chromosomal sex . These findings of measurable, biological correlates directly contradict Morty's assertion that there are 'no objective, material markers' for transgender identity. These differences are observable even in childhood and likely reflect a neurobiological basis for gender identity.11
Genetic research has also identified several genes that may play a role in gender identity development, such as polymorphisms in the androgen receptor and estrogen receptor genes.12 While there is no singular "transgender gene," these findings suggest that genetic factors can influence an individual's experienced gender identity. Variations in prenatal hormone exposure are another biological factor thought to contribute to gender diversity.13
Major medical organizations, including the American Academy of Pediatrics, American Psychological Association, and Endocrine Society, have issued statements affirming that gender identity is a real and valid aspect of human diversity with biological underpinnings.141516 The medical consensus rejects the unscientific notion that gender identity can be reduced to a simple choice between two "natural kinds."
The article's attempt to invalidate transgender identities by appealing to an arbitrary philosophical distinction crumbles under the weight of scientific evidence. Gender identity is not an either/or proposition, but a multifaceted trait shaped by a complex interplay of nature and nurture. Perpetuating a false dichotomy only serves to dismiss the real experiences of transgender individuals and fuel harmful misconceptions about this vulnerable population.
1.5 Morty’s footnotes for their first section/chapter deserve a closer look:
The article's shaky argumentative foundation is further revealed by a closer examination of its footnotes.

The first footnote baldly asserts that "woman" and "adult female" are synonymous, without evidence or argument. This is a link to another one of Morty’s articles, and will be the subject of a future article debunking this reference. It seems that trans people are not the ones that do not know what a woman is after all.17

The second footnote gestures vaguely towards "studies" on female sexual fluidity, but fails to cite even one. Such vague, unsupported appeals to scientific authority are a recurring weakness in the article's references. If I keep my hand waving vague enough, I too, can say that “studies” show pretty much anything I want to be true (or false).
Footnotes 3 and 5 rely on tendentious redefinitions of "gender identity" that bear little resemblance to how the term is used by researchers and clinicians. By attacking these straw man conceptions, Morty avoids reckoning with the reality of gender identity as understood by experts. Furthermore, their assertion about how the term is used in the wild does not line up with reality. This "soul-like ‘gender identity’" rhetoric appears to be an example of a straw man fallacy - misrepresenting an opposing view in an oversimplified or exaggerated form that's easier to discredit. Rather than addressing the actual arguments for transgender identity put forward by trans people, scientists, and major medical organizations, Morty substitutes this “metaphysical belief” caricature as a stand-in for those views.
The fourth footnote makes a sweeping claim about gender categories in Samoa and Thailand, without providing any evidence of Morty's expertise in these cultures, and provides no citations to follow up to verify/validate this claim. This casual generalization does nothing to support the article's argument.
Footnote 6 goes beyond mere scholarly sloppiness into outright conspiratorial ideation. Morty's baseless speculation about the secret motives of trans activists is a revealing glimpse into the mindset behind this piece. What they fail to recognize is that, based on the same evidence and logic, the same case could be made for Gays, Lesbians, and Bisexuals as well - unless their next claim, that the brain has its homosexuality fixed (and what of bisexual people?) has no merit? Because if it does, then it is just a matter of time and technology before we can measure it. In which case, the same questions hold true.
Finally, the seventh footnote makes an oversimplified claim about the origins of homosexuality that fails to undermine the biological basis of gender identity. Morty links to Simon LeVay's book "Gay, Straight, and the Reason Why: The Science of Sexual Orientation" in support of a claim about the biological basis of homosexuality. In fact, LeVay has elsewhere written the following:
"there is no reason to doubt that transgender identities can have a biological basis."18
Moreover, the Morty's focus on LeVay's work to the exclusion of research directly addressing the biological basis of gender identity reveals a highly selective approach to evidence. Numerous studies using brain imaging, genetic analysis, and other methods have found compelling similarities between the neurobiological underpinnings of homosexuality and transgender identity.19
The article's failure to engage with this body of evidence, while accepting a biological explanation for homosexuality based on a single author's work, suggests a deep inconsistency in its application of scientific principles. This cherry-picking of sources to fit a predetermined conclusion is a hallmark of motivated reasoning, not objective inquiry.
By ignoring inconvenient research and drawing false analogies to unrelated phenomena, Morty undermines their own argument and credibility. A genuine analysis of the science of gender identity would require grappling with the full range of evidence, not just selective citations that happen to align with one's biases.
This is to say nothing of the criticism that has been levied against LeVay, and rightfully so. Morty and their article is our focus, so I will not engage with LeVay’s work directly. Suffice it to say that the most thorough critical review of LeVay’s work and his place in the history of the American eugenics movement, please see Nancy Ordover’s American Eugenics: Race, Queer Anatomy, and the Science of Nationalism, pages 57-124. Ordover notes, “Nothing in the long medicalization of homosexuality has ever displaced what came before. What we have seen instead is additive causation theories.”
More to the point of LeVay as a questionable or biased source, it is in my experience that the anti-trans pundits and shills almost always end up referencing a circular group of “experts” no matter how discredited. LeVay is no exception, as one need only to look to LeVay’s connections to Bailey, Blanchard, and others and how their theories are clearly part of a mutually beneficial arrangement to promote each others’ work and books about sexuality.
Ultimately, from these footnotes, a clear pattern emerges: the article's impressive-looking references are a Potemkin village of weak evidence, fallacious reasoning, and rhetorical misdirection. This does not bode well for the credibility of its main arguments.
2. The mischaracterization of gender dysphoria as a "culture-bound syndrome"
The article's claim that transgender identity is a "culture-bound syndrome" limited to Western society reveals a profound ignorance of the global and historical diversity of gender expression. This assertion is not only factually inaccurate but also perpetuates harmful myths about the validity and universality of transgender experiences.
Gender dysphoria is the distress that arises from an incongruence between one's gender identity and sex assigned at birth.20 It is a well-established diagnosis in the DSM-5 and ICD-11, the authoritative diagnostic manuals used by mental health professionals worldwide. The diagnostic criteria for gender dysphoria are based on decades of clinical research and expert consensus, not cultural trends or social contagion.21
Moreover, the existence of gender diverse individuals is not a modern or Western phenomenon, but a cross-cultural and historical constant. Anthropological and historical records show that the presence of third gender, two-spirit people, and other gender variant identities have existed in societies throughout history and the world.22
For example, the hijra of South Asia, the fa'afafine of Samoa, and the waria of Indonesia are all examples of traditional third gender roles that have existed for centuries, and continue to be recognized in their respective cultures.23 The Indigenous cultures of North America have long acknowledged two-spirit individuals who embody both masculine and feminine qualities.24
This cross-cultural and historical evidence demonstrates that gender diversity is not a modern Western invention, but a naturally occurring form of human variation. Studies on the prevalence of gender dysphoria and transgender identity across the world further support this:
A meta-analysis by Meier & Labuski (2013) estimated that 0.5% to 1.3% of adults globally experience gender dysphoria25
Winter et al. (2016) reviewed studies from multiple countries and found transgender identities documented in all regions surveyed 26
The gender diversity of non-Western cultures belies the notion that being transgender is a uniquely Western "culture-bound syndrome." The fact that gender variant identities have independently arisen in so many different societies strongly suggests that gender diversity is a fundamental aspect of the human experience, not a cultural or historical aberration.27
The article's attempt to dismiss transgender identities as a culture-specific delusion stems from a parochial and ahistorical view of human gender diversity. It ignores the rich tapestry of gender expressions that have existed across cultures and eras, in order to prop up a simplistic binary view of gender that is increasingly at odds with both scientific evidence and lived experience.
These findings thoroughly refute the article's claim that gender dysphoria and transgender identity are culture-bound syndromes. The scientific evidence shows that gender diversity is a universal aspect of humanity, not a social contagion or delusion specific to the contemporary West. By denying this reality, the article reveals its underlying bias and disregard for fact.
The existence of gender diverse individuals across cultures and throughout history thoroughly debunks the article's attempt to paint being transgender as some kind of modern Western "craze."
3. The Dismissal of Transgender Identities as a "social contagion"
One of the most pernicious and harmful tropes in the article is the suggestion that transgender identities are a "social contagion" spreading through peer influence and social media. This claim is not only deeply invalidating to trans people's lived experiences but also contradicted by scientific evidence.
Social contagion refers to the spread of behaviors, attitudes or affect through imitation and conformity within a cohesive group.28 While social contagion theory has some applications in understanding collective behaviors, it is a completely inappropriate and misleading framework for conceptualizing transgender identities.
Gender identity is a deeply felt, intrinsic sense of oneself that develops in early childhood, not something that can be "caught" from others.29 The growing visibility of transgender people in recent years is not evidence of a new social contagion, but rather the result of increasing social acceptance allowing more trans people to live authentically.
The historical and cross-cultural evidence of gender diversity thoroughly refutes the notion that transgender identities are a modern social contagion. Trans and gender non-conforming people have existed in societies around the world for centuries, long before the rise of social media.30 What's new is not transgender people, but the growing mainstream awareness of their existence.
Labeling transgender identities a social contagion is not only factually baseless but also incredibly damaging to trans people's mental health and well-being. Research consistently shows that affirming trans people's identities and supporting their transition significantly improves psychological outcomes and reduces suicide risk.3132
In contrast, dismissing someone's gender identity as a "social contagion" is a form of conversion therapy that tries to change a person's gender to fit societal expectations. All major medical organizations condemn conversion therapy as ineffective and unethical due to the severe harms it causes.33
Perpetuating the social contagion myth contributes to the stigma, discrimination and violence that transgender people already face at alarming rates.34 It encourages parents to reject their trans children, politicians to limit trans people's access to healthcare, and the public to see trans people as mentally ill and delusional.
We must reject the pseudoscientific notion that transgender identities are a social contagion in favor of the empirical evidence that they are a normal and natural form of human diversity. Accepting and affirming trans people's self-determined identities is essential for their health, equality and human rights.
4. The Conflation of Gender Identity with Sexual Orientation and Paraphilias
The article's attempt to equate transgender identities with sexual orientation and paraphilias is a fundamental conceptual error that has no basis in scientific fact. Gender identity, sexual orientation, and paraphilias are distinct aspects of human diversity that may be related but are not equivalent or interchangeable.35
Gender identity refers to a person's deep-seated identification as male, female, or another gender. It is a core aspect of self that typically develops in early childhood and remains stable throughout life.36 Sexual orientation describes patterns of sexual and romantic attraction to others (e.g. straight, gay, bisexual, etc). Paraphilias are atypical sexual interests in objects, situations, or individuals.37
A person's gender identity is independent from their sexual orientation. Trans people, like cisgender people, may be straight, gay, bisexual, asexual or any other orientation. A trans woman who is exclusively attracted to men is a straight woman, not a gay man. A trans man attracted to other men is a gay man, not a straight woman.38
The article's reliance on Ray Blanchard's outdated autogynephilia theory to characterize trans women as "paraphilic men" is particularly egregious. Blanchard proposed that all trans women fit into two categories: androphilic (exclusively attracted to men) and autogynephilic (sexually aroused by the idea of being a woman).39
However, the theory has been extensively criticized for its poor scientific rigor, reliance on gender stereotypes, and failure to match the lived experiences of most trans women.40 Blanchard's own research found that many trans women did not fit their proposed typology.41 Autogynephilia is not recognized as a valid diagnosis by the DSM-5 or ICD-11.42
Moreover, the theory's core assumption that trans women's identities are rooted in sexual fetishism is contradicted by evidence that gender identity solidifies well before the development of sexual orientation in children.43 Many trans women report knowing their gender identity from a very young age, long before experiencing any sexual thoughts or desires.44
The scientific consensus rejects autogynephilia theory as an inaccurate and misleading explanation for transgender identities.45 By continuing to promote this discredited theory and conflate gender identity with sexual orientation, the article spreads damaging misconceptions that dehumanize trans people and dismiss their authentic self-knowledge.
5. The Fearmongering About Medical Transition for Transgender Youth
One of the most inflammatory sections of the article is its fearmongering portrayal of gender-affirming medical care for transgender youth. Morty paints a lurid picture of "children being castrated" and "14 year-olds getting double mastectomies," suggesting that affirming care is a form of child abuse. In reality, the standards of care for transgender minors are far more cautious, incremental, and evidence-based than the article implies.
The World Professional Association for Transgender Health (WPATH) Standards of Care, which are endorsed by the American Academy of Pediatrics, the Endocrine Society, and other major medical organizations, outline a staged approach to treatment for gender dysphoria in minors.46 The first line of care is social transition and mental health support, not medical interventions.
For youth who have reached Tanner Stage 2 of puberty (typically around age 10-11), puberty blockers may be prescribed to delay the development of secondary sex characteristics.47 Puberty blockers are safe and fully reversible – if discontinued, endogenous puberty resumes.48 This treatment is associated with reduced depression, anxiety and suicidality in trans youth.49
Hormone therapy (estrogen or testosterone) may be prescribed in mid-adolescence (age 14-16) for youth who have a persistent, well-documented gender identity and have undergone mental health evaluation.50 Genital surgeries are not performed on minors, and chest surgery is only rarely performed on older adolescents (age 16+) who meet strict eligibility criteria.51
Longitudinal research has found that access to pubertal suppression and gender-affirming hormones is associated with improved mental health outcomes and quality of life for transgender youth, with no adverse effects on bone mineralization, cognitive development, or fertility.525354 Youth denied access to affirming care are at elevated risk of depression, self-harm, and suicide attempts.55
Contrary to the article's claims, gender-affirming care does not "rush" children into transition or "cement" a transgender identity. The standards of care follow a cautious, staged approach that allows youth to explore their identity at their own pace with psychological support.56 For prepubescent children, transition is entirely social – no medical interventions are offered before puberty.
The claim that most gender non-conforming children will "desist" and identify as cisgender if not affirmed has been thoroughly debunked.57 The desistance myth is based on flawed studies that did not properly distinguish between gender non-conformity and gender dysphoria in prepubescent children.58 Youth who have a persistent cross-gender identification are likely to maintain a transgender identity, regardless of social transition.59
All major medical organizations reject "gender-exploratory therapy" or "watchful waiting" as outdated and unethical practices that deny necessary care to transgender youth.6061 So-called "exploratory therapy" is a form of conversion therapy that attempts to discourage or suppress a child's transgender identity.62 Decades of research have found such practices to be ineffective and psychologically damaging.63
The scientific consensus is clear: affirming transgender youth's identities and supporting their access to evidence-based medical transition improves mental health outcomes and saves lives.64 Spreading misinformation and unfounded fears about gender-affirming care contributes to the stigma, discrimination, and barriers to treatment that harm transgender youth. We must trust the expertise of medical professionals, not scaremongering propaganda, when it comes to the health and well-being of transgender children.
Exposing the Article's House of Cards: The Logical Fallacies Propping Up Transphobia
In addition to its many factual inaccuracies, the article is rife with logical fallacies that undermine the credibility of its arguments. Morty repeatedly relies on flawed reasoning to make sweeping generalizations, dismiss counter-evidence, and stoke fears about the supposed dangers of transgender acceptance. As there are so many, I will not address every single one, so let's examine some of the most egregious examples together. I tried to pick an example or two from each major category:
Slippery Slope: Morty argues that affirming transgender children will inevitably lead to "toddlers and babies getting mastectomies and genital surgeries," "children being castrated," and "a world of hormonal and surgical experimentation on kids." This is a classic slippery slope fallacy that assumes, without evidence, that a relatively benign action (supporting trans youth) will lead to a cascade of increasingly catastrophic outcomes.65 In reality, the standards of care for transgender minors are far more cautious and incremental than Morty suggests, and there is no push to perform genital surgeries on young children.66
No True Scotsman: Morty claims that "true transsexuals" with "actual gender dysphoria" are "a tiny sliver of a fraction of a percent of the population," dismissing the vast majority of trans-identified people as "not really transgender." This is a "no true Scotsman" fallacy that attempts to preserve a generalization by arbitrarily excluding counter-examples.67 Here, Morty defines "true" trans people so narrowly as to render the category meaningless, ignoring the diversity of transgender experiences and identities. The scientific consensus recognizes that transgender people represent a small but significant minority of the population, not a vanishingly rare exception.68 The idea here is two-fold; on one hand, the numbers are so small as to cast clouds of suspicion on the majority, and on the other hand the numbers are so small we can paint with a broad brush.
This requires holding two opposing contradictory views as being true. That trans people are so few in number as to be insignificant, while at the same time making the case that trans people are a real viable threat/concern. One precludes the other.
Appeal to Nature: Throughout the article, Morty asserts that sex is an immutable biological reality and that attempts to transcend or redefine it are a "denial of material reality." This is a fallacious appeal to nature that assumes that what occurs in nature (in this case, sexual dimorphism) is inherently good, right, or inevitable.69 However, the existence of intersex conditions, the biological evidence for transgender identities, and the wide diversity of sex and gender systems across cultures all challenge the notion that a strict male/female binary is "natural" or universal.70 Moreover, humans transcend and reshape the "natural" all the time through technology and social progress.
The manner in which Morty frames this takes on a few different aspects. The one that I found most interesting was their appeal to nature when it came to being gay vs. trans. This requires holding two opposing contradictory views as being true; that gay people are inescapably gay due to prevailing biological and scientific theories, while dismissing that trans people also fall into the same scope of causal means. Somehow Morty dismisses all the mounting evidence71 that supports trans people with these same theories as false, and ignored the fact that the brain studies they rely on were investigated and pioneered specifically for trans people in the first place - using gay and lesbian test cases as an interesting corollary and contrast against cis-heteronormative controls.72
Straw Man: So. Many. Straw men. Morty repeatedly mischaracterizes the beliefs and goals of the transgender rights movement, claiming that trans activists want to "abolish biological sex," "erase women," and "teach children they can choose their sex." These are classic straw man fallacies that involve exaggerating, misrepresenting, or oversimplifying an opponent's argument to make it easier to attack.73 Most trans advocates do not deny biological sex, but rather argue that gender identity is a separate, equally valid category.74 They seek inclusion and equality, not the erasure of women or the imposition of an ideology on children.
Ad Hominem: Like the straw men, the numbers of attacks, either pointed, barbed, or broad, are numerous. Rather than engaging with the arguments and evidence presented by transgender people and advocates, Morty resorts to attacking their character and motives. Trans women are dismissed as "perverted men" and "predators," while parents and doctors who support trans youth are accused of "child abuse" and "medical experimentation." These ad hominem fallacies attempt to discredit the person making the argument, rather than addressing the substance of their claims.75 Such hostile generalizations not only fail to advance Morty's case, but also contribute to the stigma and discrimination faced by an already marginalized population.
The cumulative effect of these fallacies is to create an emotionally charged, us-vs-them narrative that clouds reason and obscures the real issues at stake. By relying on such flawed logic, Morty reveals the underlying bias and agenda behind the article's seemingly rational facade. Readers should be wary of any argument that leans so heavily on manipulation and misdirection rather than facts and evidence.
Hasty Generalization: Morty uses individual cases of detransition to make broad claims about all trans healthcare and draws conclusions about all trans people based on a subset of cases. This is a hasty generalization because it extrapolates from a small, unrepresentative sample to make sweeping claims about a diverse population. The facts that refute this claim are covered in greater detail in the section below with the header “The uncited assertions about desistance, detransition and regret rates”
False Equivalence: Morty compares gender-affirming care to NXIVM cult brandings and FGM, equates transgender healthcare with ritual/religious practices, and draws parallels between gender identity and the goth subculture. This is a false equivalence fallacy because it compares fundamentally different things as if they were equivalent. Gender-affirming care is evidence-based medicine supported by major medical organizations, while cult brandings and FGM are non-consensual practices with no medical benefit. I think the difference between goth subculture and gender identity stands to reason. The comparison ignores crucial differences in consent, medical necessity, and scientific basis.
Post Hoc Fallacy: Morty argues that because some people experience distress after identifying as trans, the trans identity must have caused the distress, and suggests that because gender clinics emerged around the same time as increased trans visibility, they must be causing it. This is a post hoc fallacy because it assumes causation from correlation. Research shows that distress in trans individuals is often caused by societal rejection and lack of support, not by the identity itself. The increase in gender clinics reflects growing recognition and acceptance of trans people, not causation of trans identities.
Genetic Fallacy: Morty dismisses gender identity concepts because of their alleged origins in certain groups and rejects ideas based on who proposed them rather than their merit. This is a genetic fallacy because it attacks the source of an idea rather than its substance. The validity of gender identity as a concept should be evaluated based on current scientific evidence and understanding, not its historical origins or early proponents.
Inaccuracies and Falsehoods
The myth that being transgender is a new "trend" with no historical basis
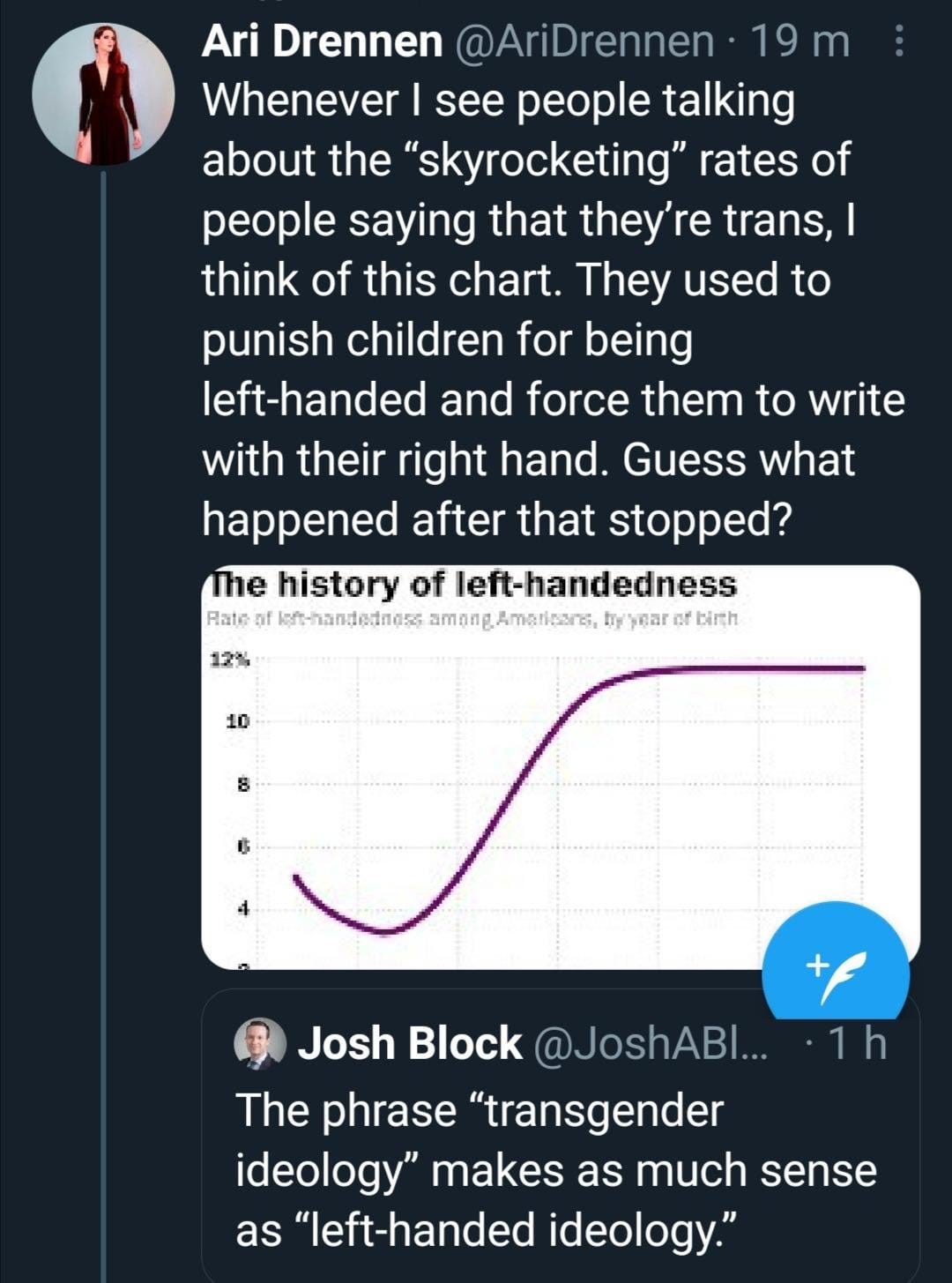
One of the most pernicious myths promoted by the article is the notion that transgender identities are a novel "trend" with no historical precedent. In reality, gender diverse people have existed in cultures worldwide throughout recorded history. In Indigenous North American societies, two-spirit individuals who embodied both masculine and feminine qualities were recognized and respected.76 The hijra of South Asia, the fa'afafine of Samoa, and the kathoey of Thailand are all examples of traditional third gender roles that have existed for centuries.77 In the Western world, figures like the Chevalier d'Éon, who presented as both male and female in 18th century France, demonstrate a long history of gender variance.78 While the language and visibility of transgender identities have evolved, they are far from a modern invention. We can also look at what happened when left-handed people were no longer considered “wrong” and a thing to be “corrected.” There was a dramatic increase in left-handed people due to social acceptance and understanding. A similar phenomenon is being witnessed since the 2010’s or so, but with trans people feeling free and with more support to come out instead of remain in the closet. We had a similar effect leading up to marriage equality with the number of gay people coming out. As Julia Serano explains:
The false claim that transition-related care is dangerous and experimental
The article's fearmongering about the supposed dangers of transition-related care has no basis in scientific fact. The standards of care for transgender health, developed by the World Professional Association for Transgender Health (WPATH), are based on decades of clinical research and experience.80 Numerous studies have found that access to medical transition significantly improves mental health outcomes and quality of life for transgender people.81 A 2018 systematic review concluded that hormone therapy is a safe and effective treatment for gender dysphoria, with a low risk of adverse events.82 Transition is not an "experiment," but a well-established medical intervention endorsed by major health organizations worldwide.83
The conspiracy theory that "gender ideology" is taking over medicine
The article's claims of a "gender ideology" pushing a "political agenda" in medicine are a baseless conspiracy theory. The growing acceptance of transgender identities in healthcare is driven by scientific evidence, not ideology. Numerous studies have found biological underpinnings for gender identity, including genetic links and brain differences between transgender and cisgender individuals.84 Major medical associations recognize the validity of transgender identities based on this evidence, not political pressure.85 The term "gender ideology" is an ideological label used to dismiss inconvenient research findings and paint transgender affirmation as extremism.86 In reality, it is the scientific consensus that has shifted in light of accumulating evidence.
The misgendering and erasure of historical trans and gender diverse figures
In its efforts to paint transgender identities as a modern delusion, the article engages in blatant misgendering and erasure of prominent gender non-conforming historical figures. Trans women like Marsha P. Johnson and Sylvia Rivera, pioneers of the LGBTQ rights movement, are dismissed as "men in dresses." Morty pointedly refers to jazz musician Billy Tipton as "she" and "a woman who lived as a man," ignoring Tipton's lifelong male identity.87 This erasure extends to gender diverse figures across cultures, from the Hijra to two-spirit people to the Chevalier d'Éon. By imposing a strict gender binary on the past, the article denies the long and varied history of trans and non-binary identities.
The uncited assertions about desistance, detransition and regret rates
Finally, the article makes a number of uncited and misleading claims about the prevalence of desistance (identifying as cisgender after previously identifying as transgender), detransition (reversing or discontinuing transition), and transition regret. Morty asserts that "60-90% of gender dysphoric children desist at puberty," that "detransitioners are starting to come out of the woodwork," and that "transition regret is common." In reality, the research shows far lower rates. Modern studies using comprehensive diagnostic criteria find desistance rates closer to 1-3%.88 Detransition is estimated to occur in only 0.4-3.5% of trans people, with the majority citing external factors like discrimination and lack of support rather than internal regret.89 Transition regret is very rare, occurring in just 0.3-3.8% of people who medically transition.90 The article's uncited claims are a gross distortion of the available evidence.
From historical erasure to scientific distortions to baseless conspiracy theories, the article's many inaccuracies and falsehoods paint a misleading and fearmongering picture of transgender realities. By examining the facts and evidence behind each of these claims, we can debunk the sensationalism and scaremongering to reveal the true diversity and validity of trans identities and experiences.
Prejudice and Bigotry, Homophobia Recycled
Furthermore, though clever in it’s use of this rhetoric and keeping an almost rational tone throughout, I was mentally checking off a list of common TERF talking points in my mind as I read Morty’s manifesto. Though many have often remarked that they are just recycled bigoted talking points,91 I decided to use Morty’s article to create a comparison of arguments from their article, to anti-gay talking points of yore.
Let’s take a look at what shook out from that analysis:
As this table shows, the anti-trans arguments in the article bear an uncanny resemblance to the homophobic rhetoric of the past. From denying the biological basis of queer identities to portraying them as a danger to children and society, the same fearmongering tactics and stereotypes are recycled and repurposed.
The language of "social contagion," "grooming," and "indoctrination" is used to stoke moral panic about both trans and gay youth. The specter of regret and detransition is wielded to undermine bodily autonomy, just as "ex-gay" narratives were used to justify conversion therapy. The entire framing of LGBTQ identities as a "craze" or "ideology" that threatens social order and must be stopped at all costs is a common thread.
While the specific contexts and experiences of gay and trans people are distinct, the rhetorical strategies used to attack them are remarkably similar. This reveals the adaptable nature of anti-LGBTQ bigotry, which evolves to target the most marginalized subgroups as past arguments lose legitimacy in the mainstream.
By recognizing these parallels, we can more effectively counter anti-trans propaganda as a repackaging of discredited homophobic myths. We must learn from the hard-fought victories of the gay rights movement and stand firm against the demonization of trans people, especially youth. These recycled tropes have no more validity when leveled against trans people today than they did against lesbians and gays in decades past. It's time to consign them to the dustbin of history once and for all.
Wrapping It All Up
In this comprehensive debunking, we have systematically dismantled the many false claims, flawed arguments, and misleading narratives that comprise this article's anti-transgender propaganda. From its reliance on biological essentialism to its dismissal of trans identities as a "social contagion," from its fearmongering about medical transition to its historical revisionism, we have exposed the intellectual bankruptcy and ideological bias at the heart of this piece.
But this is about more than just refuting bad arguments. It's about challenging the real-world harms that this kind of misinformation inflicts on transgender people, especially youth. Propaganda like this article contributes to a climate of ignorance, fear and hostility that threatens trans people's mental health, physical safety and fundamental rights. It emboldens bullies, undermines support systems, and justifies discrimination. This is of particular importance due to recent events and the perception of a majority shift and turn in politics, and with it the increased threat to minorities - particularly the anti-trans targeted propaganda.
That's why it's so important that we continue to debunk these myths and fight back against this dangerous rhetoric. We must counter lies with facts, pseudoscience with real research, and prejudice with empathy. The evidence is clear: being transgender is a normal and natural form of human diversity, not a delusion or disorder. Transgender identities are real, valid and worthy of respect, especially in youth who deserve to be supported and affirmed, not demonized and discouraged.
Ultimately, we need to push for a world where this kind of anti-trans propaganda is relegated to the dustbin of history, and where every person's gender identity is accepted as an integral part of who they are. This means advocating for greater understanding and acceptance of trans people in all aspects of society, from healthcare to education to public policy. It means following the evidence and expertise of medical authorities, not the cynical machinations of political opportunists.
Most of all, it means standing in solidarity with the transgender community as they continue to demonstrate resilience, courage and pride in the face of ongoing attacks on their basic humanity. Trans people have always existed and resisted, forming communities of mutual support and fighting back against those who would deny their right to live authentically. In a world still filled with ignorance and injustice, their persistence and power is a beacon of hope for us all.
So let this debunking be a call to action and a declaration of allyship. In exposing the lies of anti-trans ideologues, may we commit to uplifting the voices and experiences of actual trans people. In the face of animosity and aggression, may we respond with acceptance and affirmation. In a society still plagued by transmisia, may we have the courage to confront it wherever we find it. Because in the end, the struggle for trans liberation is inseparable from the universal struggle for human rights, dignity and freedom. And that is a cause we can all fight for and believe in.
Do not despair, do not give up, do not panic-

ORGANIZE!
Morty, A. (20241025). The war to annihilate sex. Substack. https://artymorty.substack.com/p/the-war-to-annihilate-sex
The War to Annihilate Sex - Arty Morty's Substack ↩Morty, A. (n.d.). Arty Morty's Substack. Substack.
https://artymorty.substack.com/ ↩Morty, A. (n.d.). About - Arty Morty's Substack. Substack. https://artymorty.substack.com/about ↩
O'Malley, S., & Ayad, S. (Hosts). (n.d.). Feminine boy to gay man: A conversation with Arty Morty [Episode 3]. In Gender: A Wider Lens. [Video].YouTube.
Link: www.youtube.com/watch?v=O-THqe2_0XE ↩Transgender Map. (20240117). “Arty Morty” vs. transgender people. https://www.transgendermap.com/issues/topics/media/arty-morty/ ↩
Morty, A. (2021) “Anyone still trying to convince themself that…”. Tweet. Twitter. https://twitter.com/artymortyarty/status/1375180897629114373 ↩
Morty, A. (20230623). Let the right one in: Who is — and isn't — trans? Substack. https://artymorty.substack.com/p/let-the-right-one-in-who-is-and-isnt ↩
Morty, A. (2024). Trans activists vs. Scientologists! The similarities are uncanny [Video].YouTube. Link: https://www.youtube.com/watch?v=TcqqGJrCpFY ↩
Mazzuca, C., Majid, A., Lugli, L., Nicoletti, R., & Borghi, A. M. (2020, March 31). Gender is a multifaceted concept: evidence that specific life experiences differentially shape the concept of gender. https://doi.org/10.31219/osf.io/ugv43 ↩
Guillamon, A., Junque, C., & Gómez-Gil, E. (2016). A Review of the Status of Brain Structure Research in Transsexualism. Archives of Sexual Behavior, 45(7), 1615–1648. https://doi.org/10.1007/s10508-016-0768-5 ↩
Olson, K. R. (2017). Prepubescent Transgender Children: What We Do and Do Not Know. Journal of the American Academy of Child & Adolescent Psychiatry, 56(3), 155–156.e3. 10.1016/j.jaac.2015.11.015 https://doi.org/10.1016/j.jaac.2016.11.015 ↩
Fernández, R., Guillamon, A., Cortés-Cortés, J., Gómez-Gil, E., Jácome, A., Esteva, I., Almaraz, M. C., Mora, M., Aranda, G., & Pásaro, E. (2018). Molecular basis of Gender Dysphoria: Androgen and estrogen receptor interaction. Psychoneuroendocrinology, 98, 161–167. https://doi.org/10.1016/j.psyneuen.2018.07.032 ↩
Roselli, C. E. (2018). Neurobiology of gender identity and sexual orientation. Journal of Neuroendocrinology, 30(7), e12562. https://doi.org/10.1111/jne.12562 ↩
Rafferty, J., Committee on Psychosocial Aspects of Child and Family Health, Committee on Adolescence, & Section on Lesbian, Gay, Bisexual, and Transgender Health and Wellness. (2018). Ensuring Comprehensive Care and Support for Transgender and Gender-Diverse Children and Adolescents. Pediatrics, 142(4). https://doi.org/10.1542/peds.2018-2162 ↩
American Psychological Association. (2015). Guidelines for Psychological Practice with Transgender and Gender Nonconforming People. American Psychologist, 70(9), 832–864. https://doi.org/10.1037/a0039906 ↩
Hembree, W. C., Cohen-Kettenis, P. T., Gooren, L., Hannema, S. E., Meyer, W. J., Murad, M. H., Rosenthal, S. M., Safer, J. D., Tangpricha, V., & T'Sjoen, G. G. (2017). Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society Clinical Practice Guideline. The Journal of Clinical Endocrinology & Metabolism, 102(11), 3869–3903. https://doi.org/10.1210/jc.2017-01658 ↩
PITT. “What is a woman?” (202411) Substack. People with Inconvenient Truth about Transphobes. Q&A Section. https://pittpeople.substack.com/p/what-is-a-woman ↩
LeVay, S., Baldwin, J. I., & Baldwin, J. D. (2019). Discovering human sexuality (Fourth edition). Sinauer Associates ; Imprint of Oxford University Press. ↩
See, for example:
Guillamon et al. (2016), Archives of Sexual Behavior, 45(7), 1615-1648;
Altinay & Anand (2020), Current Psychiatry Reports, 22(6), 29;
Fernández et al. (2018), Psychoneuroendocrinology, 98, 161-167;
Foreman et al. (2019), Scientific Reports, 9(1), 20099;
Roselli (2018), Journal of Neuroendocrinology, 30(7), e12562;
Balthazart (2020), Neuroscience & Biobehavioral Reviews, 111, 28-56. ↩American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (DSM-5®). American Psychiatric Pub. ↩
E. Coleman, A. E. Radix, W. P. Bouman, G. R. Brown, A. L. C. de Vries, M. B.Deutsch, R. Ettner, L. Fraser, M. Goodman, J. Green, A. B. Hancock, T. W. Johnson, D. H. Karasic,G. A. Knudson, …, M.A. West & J. Arcelus (2022) Standards of Care for the Health of Transgender and GenderDiverse People, Version 8, International Journal of Transgender Health, 23:sup1, S1-S259, DOI:10.1080/26895269.2022.2100644 ↩
Herdt, G. H. (1993). Third Sex, Third Gender: Beyond Sexual Dimorphism in Culture and History. Zone Books. ↩
Nanda, S. (1999). Neither Man nor Woman: The Hijras of India. Wadsworth Publishing Company. ↩
Jacobs, S.-E., Thomas, W., & Lang, S. (1997). Two-Spirit People: Native American Gender Identity, Sexuality, and Spirituality. University of Illinois Press. ↩
Meier, S. C., & Labuski, C. M. (2013). The demographics of the transgender population. In A. K. Baumle (Ed.), International handbook on the demography of sexuality (pp. 289–327). Springer Science + Business Media. https://doi.org/10.1007/978-94-007-5512-3_16 ↩
Winter S, Diamond M, Green J, Karasic D, Reed T, Whittle S, Wylie K. Transgender people: health at the margins of society. Lancet. 2016 Jul 23;388(10042):390-400. doi: 10.1016/S0140-6736(16)00683-8. Epub 2016 Jun 17. PMID: 27323925. ↩
Stryker, S. (2017). Transgender History: The Roots of Today's Revolution. Seal Press. ↩
Le Bon, G. (1895). The Crowd: A Study of the Popular Mind. T.F. Unwin.
Link[PDF]: https://www.files.ethz.ch/isn/125518/1414_LeBon.pdf ↩Gülgöz, S., Glazier, J. J., Enright, E. A., Alonso, D. J., Durwood, L. J., Fast, A. A., Lowe, R., Ji, C., Heer, J., Martin, C. L., & Olson, K. R. (2019). Similarity in transgender and cisgender children's gender development. Proceedings of the National Academy of Sciences, 116(49), 24480–24485. https://doi.org/10.1073/pnas.1909367116
Link[PDF]: https://www.pnas.org/doi/pdf/10.1073/pnas.1909367116 ↩Stryker, S. (2017). Transgender History: The Roots of Today's Revolution. Seal Press. ↩
Turban, J. L., King, D., Carswell, J. M., & Keuroghlian, A. S. (2020). Pubertal Suppression for Transgender Youth and Risk of Suicidal Ideation. Pediatrics, 145(2). https://doi.org/10.1542/peds.2019-1725 ↩
Bränström, R., & Pachankis, J. E. (2020). Reduction in Mental Health Treatment Utilization Among Transgender Individuals After Gender-Affirming Surgeries: A Total Population Study. American Journal of Psychiatry, 177(8), 727–734. https://doi.org/10.1176/appi.ajp.2019.19010080 ↩
WPATH. (2017). Position Statement on Medical Necessity of Treatment, Sex Reassignment, and Insurance Coverage in the U.S.A. https://www.wpath.org/media/cms/Documents/Web%20Transfer/Policies/WPATH-Position-on-Medical-Necessity-12-21-2016.pdf ↩
James, S. E., Herman, J. L., Rankin, S., Keisling, M., Mottet, L., & Anafi, M. (2016). The Report of the 2015 U.S. Transgender Survey. National Center for Transgender Equality. https://transequality.org/sites/default/files/docs/usts/USTS-Full-Report-Dec17.pdf ↩
American Psychological Association. (2015). See 15 Above ↩
Olson, K. R., Key, A. C., & Eaton, N. R. (2015). Gender Cognition in Transgender Children. Psychological Science, 26(4), 467–474. https://doi.org/10.1177/0956797614568156 ↩
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (DSM-5®). American Psychiatric Pub. ↩
O'Hara, M. E., & NPR Staff. (2021, June 2). A guide to gender identity terms. NPR. https://www.npr.org/2021/06/02/996319297/gender-identity-pronouns-expression-guide-lgbtq ↩
Blanchard, R. (1989). The concept of autogynephilia and the typology of male gender dysphoria. The Journal of Nervous and Mental Disease, 177(10), 616–623. https://doi.org/10.1097/00005053-198910000-00004 ↩
Serano, J. M. (2010). The Case Against Autogynephilia. International Journal of Transgenderism, 12(3), 176–187. https://doi.org/10.1080/15532739.2010.514223 ↩
Nuttbrock, L., Bockting, W., Mason, M., Hwahng, S., Rosenblum, A., Macri, M., & Becker, J. (2011). A Further Assessment of Blanchard's Typology of Homosexual Versus Non-Homosexual or Autogynephilic Gender Dysphoria. Archives of Sexual Behavior, 40(2), 247–257. https://doi.org/10.1007/s10508-009-9579-2 ↩
Davy, Z., & Toze, M. (2018). What Is Gender Dysphoria? A Critical Systematic Narrative Review. Transgender Health, 3(1), 159–169. https://doi.org/10.1089/trgh.2018.0014 ↩
Olson, K. R. (2016). See 11 Above ↩
Turban, J. L., & Ehrensaft, D. (2018). Research Review: Gender identity in youth: Treatment paradigms and controversies. Journal of Child Psychology and Psychiatry, 59(12), 1228–1243. https://doi.org/10.1111/jcpp.12833 ↩
Bockting, W., Knudson, G., & Goldberg, J. M. (2006). Counseling and Mental Health Care for Transgender Adults and Loved Ones. International Journal of Transgenderism, 9(3–4), 35–82. https://doi.org/10.1300/J485v09n03_03 ↩
Coleman, E. SOC-8. See 21 Above ↩
Hembree, W. C., Cohen-Kettenis, P. T., Gooren, L., Hannema, S. E., Meyer, W. J., Murad, M. H., Rosenthal, S. M., Safer, J. D., Tangpricha, V., & T'Sjoen, G. G. (2017). See 16 Above. ↩
Rafferty, J., Committee on Psychosocial Aspects of Child and Family Health, Committee on Adolescence, & Section on Lesbian, Gay, Bisexual, and Transgender Health and Wellness. (2018). See 14 Above. ↩
Turban, J. L., King, D., Carswell, J. M., & Keuroghlian, A. S. (2020). See 31 Above ↩
Hembree et al. (2017). See 47 Above ↩
Rafferty et al. (2018). See 48 Above ↩
de Vries, A. L. C., McGuire, J. K., Steensma, T. D., Wagenaar, E. C. F., Doreleijers, T. A. H., & Cohen-Kettenis, P. T. (2014). Young Adult Psychological Outcome After Puberty Suppression and Gender Reassignment. Pediatrics, 134(4), 696–704. https://doi.org/10.1542/peds.2013-2958 ↩
Vlot, M. C., Klink, D. T., den Heijer, M., Blankenstein, M. A., Rotteveel, J., & Heijboer, A. C. (2017). Effect of pubertal suppression and cross-sex hormone therapy on bone turnover markers and bone mineral apparent density (BMAD) in transgender adolescents. Bone, 95, 11–19. https://doi.org/10.1016/j.bone.2016.11.008 ↩
Mahfouda, S., Moore, J. K., Siafarikas, A., Zepf, F. D., & Lin, A. (2017). Puberty suppression in transgender children and adolescents. The Lancet Diabetes & Endocrinology, 5(10), 816–826. https://doi.org/10.1016/S2213-8587(17)30099-2 ↩
Turban et al. (2020). See 31 Above ↩
Ehrensaft, D. (2017). Gender nonconforming youth: Current perspectives. Adolescent Health, Medicine and Therapeutics, 8, 57–67. https://doi.org/10.2147/AHMT.S110859 ↩
Temple Newhook, J., Pyne, J., Winters, K., Feder, S., Holmes, C., Tosh, J., Sinnott, M.-L., Jamieson, A., & Pickett, S. (2018). A critical commentary on follow-up studies and "desistance" theories about transgender and gender-nonconforming children. International Journal of Transgenderism, 19(2), 212–224. https://doi.org/10.1080/15532739.2018.1456390 ↩
Olson, K. R. (2016). See 11 Above ↩
Steensma, T. D., McGuire, J. K., Kreukels, B. P. C., Beekman, A. J., & Cohen-Kettenis, P. T. (2013). Factors associated with desistence and persistence of childhood gender dysphoria: A quantitative follow-up study. Journal of the American Academy of Child & Adolescent Psychiatry, 52(6), 582–590. https://doi.org/10.1016/j.jaac.2013.03.016 ↩
American Psychological Association. (2015). See 15 Above ↩
Rafferty et al. (2018). See 48 Above ↩
SAMHSA. (2015). Ending Conversion Therapy: Supporting and Affirming LGBTQ Youth. Substance Abuse and Mental Health Services Administration. https://store.samhsa.gov/product/Ending-Conversion-Therapy-Supporting-and-Affirming-LGBTQ-Youth/SMA15-4928 ↩
WPATH. (2017). See 33 Above ↩
Turban, J. L., & Ehrensaft, D. (2018). See 44 Above ↩
Walton, D. (2015). The Basic Slippery Slope Argument. Informal Logic, 35(3), 273–311. https://doi.org/10.22329/il.v35i3.4286 ↩
Coleman, E. SOC-8. See 21 Above ↩
Sinnott-Armstrong, W. (2018). Think Again: How to Reason and Argue (pp. 182-183). Penguin. ↩
Flores, A. R., Herman, J. L., Gates, G. J., & Brown, T. N. T. (2016). How Many Adults Identify as Transgender in the United States? The Williams Institute. https://williamsinstitute.law.ucla.edu/publications/trans-adults-united-states/ ↩
Moore, G. E. (1903). Principia Ethica. Cambridge University Press. ↩
Ainsworth, C. (2015). Sex redefined. Nature, 518(7539), 288–291. https://doi.org/10.1038/518288a ↩
These three studies, for example:
Polderman TJC, Kreukels BPC, Irwig MS, Beach L, Chan YM, Derks EM, Esteva I, Ehrenfeld J, Heijer MD, Posthuma D, Raynor L, Tishelman A, Davis LK; International Gender Diversity Genomics Consortium. The Biological Contributions to Gender Identity and Gender Diversity: Bringing Data to the Table. Behav Genet. 2018 Mar;48(2):95-108. doi: 10.1007/s10519-018-9889-z. Epub 2018 Feb 19. PMID: 29460079.
early brain studies on transgender people did predate and inform later work on sexual orientation. Pioneering research by Zhou et al. (1995) and Kruijver et al. (2000) first identified differences in brain structures between transgender and cisgender individuals. This work was extended to sexual orientation by researchers like Swaab, Hofman, LeVay and others in the late 1990s and 2000s (Swaab & Hofman, 1990; LeVay, 1991; Savic & Lindström, 2008). ↩
Talisse, R., & Aikin, S. (2006). Two Forms of the Straw Man. Argumentation, 20(3), 345–352. https://doi.org/10.1007/s10503-006-9017-8 ↩
Serano, J. (2007). Whipping Girl: A Transsexual Woman on Sexism and the Scapegoating of Femininity. Seal Press. ↩
Bondy, P. (2015). Virtues, evidence, and ad hominem arguments. Informal Logic, 35(4), 450–466. https://doi.org/10.22329/il.v35i4.4330 ↩
Jacobs, S. E., Thomas, W., & Lang, S. (Eds.). (1997). See 24 Above ↩
Nanda, S. (1999). See 23 Above ↩
Decker, M. (2014). The Chevalier d'Éon and his worlds: Gender, espionage and politics in the eighteenth century. Bloomsbury Publishing. ↩
Serano, J. (2017) Transgender Agendas, Social Contagion, Peer Pressure, and Prevalence. Medium. https://juliaserano.medium.com/transgender-agendas-social-contagion-peer-pressure-and-prevalence-c3694d11ed24 ↩
Coleman, E. SOC-8. See 21 Above ↩
Murad, M. H., Elamin, M. B., Garcia, M. Z., Mullan, R. J., Murad, A., Erwin, P. J., & Montori, V. M. (2010). Hormonal therapy and sex reassignment: A systematic review and meta‐analysis of quality of life and psychosocial outcomes. Clinical endocrinology, 72(2), 214-231. https://pubmed.ncbi.nlm.nih.gov/19473181/ ↩
Weinand, J. D., & Safer, J. D. (2015). Hormone therapy in transgender adults is safe with provider supervision; a review of hormone therapy sequelae for transgender individuals. Journal of clinical & translational endocrinology, 2(2), 55-60. https://pmc.ncbi.nlm.nih.gov/articles/PMC5226129/ ↩
American Medical Association. (2019). Health insurance coverage for gender-affirming care of transgender patients. https://www.ama-assn.org/system/files/2019-03/transgender-coverage-issue-brief.pdf ↩
Polderman, T. J., Kreukels, B. P., Irwig, M. S., Beach, L., Chan, Y. M., Derks, E. M., ... & Davis, L. K. (2018). The biological contributions to gender identity and gender diversity: Bringing data to the table. Behavior genetics, 48(2), 95-108. https://pubmed.ncbi.nlm.nih.gov/29460079/ ↩
American Psychological Association. (2015). See 15 Above ↩
Serano, J. (2020). Debunking "Trans Women Are Not Women" Arguments. Medium. https://juliaserano.medium.com/debunking-trans-women-are-not-women-arguments-85fd5ab0e19c ↩
Middlebrook, D. W. (1999). Suits me: The double life of Billy Tipton. Virago. ↩
Temple Newhook, J., Pyne, J., Winters, K., Feder, S., Holmes, C., Tosh, J., ... & Pickett, S. (2018). See 57 Above. ↩
James, S. E., Herman, J. L., Rankin, S., Keisling, M., Mottet, L., & Anafi, M. (2016). See 34 Above ↩
Wiepjes, C. M., Nota, N. M., de Blok, C. J., Klaver, M., de Vries, A. L., Wensing-Kruger, S. A., ... & den Heijer, M. (2018). The Amsterdam cohort of gender dysphoria study (1972–2015): trends in prevalence, treatment, and regrets. The Journal of Sexual Medicine, 15(4), 582-590. https://pubmed.ncbi.nlm.nih.gov/29463477/ ↩
I even wrote a time-lapsed article illustrating this recycle bigotry using the current “bathroom panic” issue and working backwards in time. I thought it was a novel approach - give it a read!
PITT. “The Trans Takeover Begins!”. Substack.
https://pittpeople.substack.com/p/the-trans-takeover-begins ↩
Kreukels BP, Guillamon A. Neuroimaging studies in people with gender incongruence. Int Rev Psychiatry. 2016;28(1):120-8. doi: 10.3109/09540261.2015.1113163. Epub 2016 Jan 14. PMID: 26766406.
Theisen JG, Sundaram V, Filchak MS, Chorich LP, Sullivan ME, Knight J, Kim HG, Layman LC. The Use of Whole Exome Sequencing in a Cohort of Transgender Individuals to Identify Rare Genetic Variants. Sci Rep. 2019 Dec 27;9(1):20099. doi: 10.1038/s41598-019-53500-y. PMID: 31882810; PMCID: PMC6934803. ↩
early brain studies on transgender people did predate and inform later work on sexual orientation. Pioneering research by Zhou et al. (1995) and Kruijver et al. (2000) first identified differences in brain structures between transgender and cisgender individuals. This work was extended to sexual orientation by researchers like Swaab, Hofman, LeVay and others in the late 1990s and 2000s (Swaab & Hofman, 1990; LeVay, 1991; Savic & Lindström, 2008). ↩
Talisse, R., & Aikin, S. (2006). Two Forms of the Straw Man. Argumentation, 20(3), 345–352. https://doi.org/10.1007/s10503-006-9017-8 ↩
Serano, J. (2007). Whipping Girl: A Transsexual Woman on Sexism and the Scapegoating of Femininity. Seal Press. ↩
Bondy, P. (2015). Virtues, evidence, and ad hominem arguments. Informal Logic, 35(4), 450–466. https://doi.org/10.22329/il.v35i4.4330 ↩
Jacobs, S. E., Thomas, W., & Lang, S. (Eds.). (1997). See 24 Above ↩
Nanda, S. (1999). See 23 Above ↩
Decker, M. (2014). The Chevalier d'Éon and his worlds: Gender, espionage and politics in the eighteenth century. Bloomsbury Publishing. ↩
Serano, J. (2017) Transgender Agendas, Social Contagion, Peer Pressure, and Prevalence. Medium. https://juliaserano.medium.com/transgender-agendas-social-contagion-peer-pressure-and-prevalence-c3694d11ed24 ↩
Coleman, E. SOC-8. See 21 Above ↩
Murad, M. H., Elamin, M. B., Garcia, M. Z., Mullan, R. J., Murad, A., Erwin, P. J., & Montori, V. M. (2010). Hormonal therapy and sex reassignment: A systematic review and meta‐analysis of quality of life and psychosocial outcomes. Clinical endocrinology, 72(2), 214-231. https://pubmed.ncbi.nlm.nih.gov/19473181/ ↩
Weinand, J. D., & Safer, J. D. (2015). Hormone therapy in transgender adults is safe with provider supervision; a review of hormone therapy sequelae for transgender individuals. Journal of clinical & translational endocrinology, 2(2), 55-60. https://pmc.ncbi.nlm.nih.gov/articles/PMC5226129/ ↩
American Medical Association. (2019). Health insurance coverage for gender-affirming care of transgender patients. https://www.ama-assn.org/system/files/2019-03/transgender-coverage-issue-brief.pdf ↩
Polderman, T. J., Kreukels, B. P., Irwig, M. S., Beach, L., Chan, Y. M., Derks, E. M., ... & Davis, L. K. (2018). The biological contributions to gender identity and gender diversity: Bringing data to the table. Behavior genetics, 48(2), 95-108. https://pubmed.ncbi.nlm.nih.gov/29460079/ ↩
American Psychological Association. (2015). See 15 Above ↩
Serano, J. (2020). Debunking "Trans Women Are Not Women" Arguments. Medium. https://juliaserano.medium.com/debunking-trans-women-are-not-women-arguments-85fd5ab0e19c ↩
Middlebrook, D. W. (1999). Suits me: The double life of Billy Tipton. Virago. ↩
Temple Newhook, J., Pyne, J., Winters, K., Feder, S., Holmes, C., Tosh, J., ... & Pickett, S. (2018). See 57 Above. ↩
James, S. E., Herman, J. L., Rankin, S., Keisling, M., Mottet, L., & Anafi, M. (2016). See 34 Above ↩
Wiepjes, C. M., Nota, N. M., de Blok, C. J., Klaver, M., de Vries, A. L., Wensing-Kruger, S. A., ... & den Heijer, M. (2018). The Amsterdam cohort of gender dysphoria study (1972–2015): trends in prevalence, treatment, and regrets. The Journal of Sexual Medicine, 15(4), 582-590. https://pubmed.ncbi.nlm.nih.gov/29463477/ ↩
I even wrote a time-lapsed article illustrating this recycle bigotry using the current “bathroom panic” issue and working backwards in time. I thought it was a novel approach - give it a read!
PITT. “The Trans Takeover Begins!”. Substack.
https://pittpeople.substack.com/p/the-trans-takeover-begins ↩
early brain studies on transgender people did predate and inform later work on sexual orientation. Pioneering research by Zhou et al. (1995) and Kruijver et al. (2000) first identified differences in brain structures between transgender and cisgender individuals. This work was extended to sexual orientation by researchers like Swaab, Hofman, LeVay and others in the late 1990s and 2000s (Swaab & Hofman, 1990; LeVay, 1991; Savic & Lindström, 2008). ↩
Talisse, R., & Aikin, S. (2006). Two Forms of the Straw Man. Argumentation, 20(3), 345–352. https://doi.org/10.1007/s10503-006-9017-8 ↩
Serano, J. (2007). Whipping Girl: A Transsexual Woman on Sexism and the Scapegoating of Femininity. Seal Press. ↩
Bondy, P. (2015). Virtues, evidence, and ad hominem arguments. Informal Logic, 35(4), 450–466. https://doi.org/10.22329/il.v35i4.4330 ↩
Jacobs, S. E., Thomas, W., & Lang, S. (Eds.). (1997). See 24 Above ↩
Nanda, S. (1999). See 23 Above ↩
Decker, M. (2014). The Chevalier d'Éon and his worlds: Gender, espionage and politics in the eighteenth century. Bloomsbury Publishing. ↩
Serano, J. (2017) Transgender Agendas, Social Contagion, Peer Pressure, and Prevalence. Medium. https://juliaserano.medium.com/transgender-agendas-social-contagion-peer-pressure-and-prevalence-c3694d11ed24 ↩
Coleman, E. SOC-8. See 21 Above ↩
Murad, M. H., Elamin, M. B., Garcia, M. Z., Mullan, R. J., Murad, A., Erwin, P. J., & Montori, V. M. (2010). Hormonal therapy and sex reassignment: A systematic review and meta‐analysis of quality of life and psychosocial outcomes. Clinical endocrinology, 72(2), 214-231. https://pubmed.ncbi.nlm.nih.gov/19473181/ ↩
Weinand, J. D., & Safer, J. D. (2015). Hormone therapy in transgender adults is safe with provider supervision; a review of hormone therapy sequelae for transgender individuals. Journal of clinical & translational endocrinology, 2(2), 55-60. https://pmc.ncbi.nlm.nih.gov/articles/PMC5226129/ ↩
American Medical Association. (2019). Health insurance coverage for gender-affirming care of transgender patients. https://www.ama-assn.org/system/files/2019-03/transgender-coverage-issue-brief.pdf ↩
Polderman, T. J., Kreukels, B. P., Irwig, M. S., Beach, L., Chan, Y. M., Derks, E. M., ... & Davis, L. K. (2018). The biological contributions to gender identity and gender diversity: Bringing data to the table. Behavior genetics, 48(2), 95-108. https://pubmed.ncbi.nlm.nih.gov/29460079/ ↩
American Psychological Association. (2015). See 15 Above ↩
Serano, J. (2020). Debunking "Trans Women Are Not Women" Arguments. Medium. https://juliaserano.medium.com/debunking-trans-women-are-not-women-arguments-85fd5ab0e19c ↩
Middlebrook, D. W. (1999). Suits me: The double life of Billy Tipton. Virago. ↩
Temple Newhook, J., Pyne, J., Winters, K., Feder, S., Holmes, C., Tosh, J., ... & Pickett, S. (2018). See 57 Above. ↩
James, S. E., Herman, J. L., Rankin, S., Keisling, M., Mottet, L., & Anafi, M. (2016). See 34 Above ↩
Wiepjes, C. M., Nota, N. M., de Blok, C. J., Klaver, M., de Vries, A. L., Wensing-Kruger, S. A., ... & den Heijer, M. (2018). The Amsterdam cohort of gender dysphoria study (1972–2015): trends in prevalence, treatment, and regrets. The Journal of Sexual Medicine, 15(4), 582-590. https://pubmed.ncbi.nlm.nih.gov/29463477/ ↩
I even wrote a time-lapsed article illustrating this recycle bigotry using the current “bathroom panic” issue and working backwards in time. I thought it was a novel approach - give it a read!
PITT. “The Trans Takeover Begins!”. Substack.
https://pittpeople.substack.com/p/the-trans-takeover-begins ↩