Twisting the Facts: How Blendr News Spreads Disinformation on Trans Youth Care
The Inconvenient Truth: Gender-Affirming Care Saves Lives
A Rebuttal to Liam DeBoer’s Article in Blendr News
Hello there PITT crew, today we are going to talk about a recent article from Blendr News that makes some very serious accusations against gender-affirming care for transgender youth. The piece, written by Liam DeBoer, claims that this widely accepted medical practice is actually "medical malpractice" and even goes so far as to call it a "crime against humanity." These are strong claims that require strong evidence, and they require a thorough examination.
The article, titled "Crimes Against Humanity: The Medical Malpractice of Gender-Affirming Care," is built upon a foundation of sensationalized language, cherry-picked anecdotes, and misrepresented research rather than a balanced, rational look at the evidence. DeBoer's piece is rife with fallacies, falsehoods and misrepresentations that paint a highly distorted picture of gender-affirming care. The reality is that when properly administered following established protocols, gender-affirming care is safe, effective and often lifesaving for transgender youth who need it. Let's dive into the claims made in the article and separate fact from fiction.
Hiding in Plain Sight: The Truth About Dr. Olson-Kennedy's Research
One of the central pieces of "evidence" cited is a New York Times investigation which reportedly found that a prominent researcher, Dr. Johanna Olson-Kennedy, "withheld crucial data" showing no mental health benefits from puberty blockers and surgeries. DeBoer presents this as a smoking gun, claiming Olson-Kennedy hid the data because it would "weaponize" the results.
However, this is a gross misrepresentation of the actual situation. As journalist Erin Reed points out in a thorough fact-check of the Times article, Olson-Kennedy and her team have published 28 peer-reviewed papers from their NIH-funded study on transgender youth, including several that look specifically at youth taking puberty blockers. The data in question was from a preliminary analysis with a small sample size. Olson-Kennedy explained that given the preliminary nature and small sample, there were concerns about the data being misinterpreted if published prematurely from an ongoing study, not concealed for nefarious reasons.1
Furthermore, Olson-Kennedy's published research has actually found that transgender youth who accessed puberty blockers earlier had better mental health outcomes compared to those who waited for hormone therapy - a key piece of context missing from the Times article and DeBoer's piece. As Reed explains, "the purpose of puberty blockers is not to 'improve' a trans youth's mental health. Gender dysphoria arises from a mismatch between a person's physical development and their internal sense of gender identity. Puberty blockers pause physical changes, ensuring that when a transgender youth is ready to begin hormone therapy, as determined by their medical team, they won't have undergone unwanted pubertal changes."2
Pressing Pause ≠ Permanent Damage: Puberty Blockers 101
Another recurring theme in DeBoer's article is the portrayal of puberty blockers as dangerous drugs that cause "irreversible damage" to youth. He claims these medications lead to "chemical castration" and that doctors are "sacrificing children" by prescribing them. The reality is that puberty blockers are considered safe, reversible medications that have been used for decades to treat precocious puberty.3 Their purpose in gender-affirming care is to temporarily delay puberty, providing time for transgender youth to explore their identity without the distress of permanent physical changes.4
It's true that like any medication, puberty blockers have potential side effects that need to be monitored, including impacts on bone density. However, as shown in a published study by Olson-Kennedy and team, transgender youth tend to have more bone density issues even before starting any treatment, likely due to lack of exercise and vitamin D. Research shows that bone loss on blockers, if it occurs, is usually minor and reversible with calcium and vitamin D supplementation.56 Contrary to DeBoer's claims, these medications give adolescents and their families time to make informed decisions, not rush them into anything.
Transition Treadmill or Personalized Care? Inside the Gender-Affirming Model
This brings us to another false narrative pushed in the article - the idea that gender-affirming care is "rushing" vulnerable youth into medical transition. DeBoer suggests that kids are being fast-tracked into taking hormones and getting surgeries, often at the behest of doctors and clinics with ideological or financial motives. The reality could not be further from the truth. The gender-affirming care model, as outlined in the standards of care7 from major medical organizations like the Endocrine Society8 and American Academy of Pediatrics, is a highly individualized process involving in-depth assessments, mental health support, and ongoing evaluation of each youth's unique circumstances and needs.9
Before any medical interventions are even considered, transgender youth undergo extensive psychological assessments to ensure they meet diagnostic criteria for gender dysphoria and rule out other mental health concerns. Counseling is provided to help youth explore their identity and determine if social transition (changing name, pronouns, clothing etc.) helps alleviate their distress. Puberty blockers are typically not prescribed until the early stages of puberty, and cross-sex hormones are not given until mid-teens at the earliest, and only for youth who have been insistent, persistent and consistent in their gender identity over time. Surgeries are not performed on minors except in very rare cases, generally not until the age of legal majority.
The notion that all transgender youth are being pushed towards medical transition is simply false. The reality is that gender-affirming care is not a one-size-fits-all conveyor belt, but a collaborative process in which each youth's individual needs are carefully considered by medical and mental health professionals along with family support. The goal is not to push anyone into a singular path, but to ease gender dysphoria and improve overall well-being, which for some may involve medical interventions, but for many others does not.
"ROGD" Repackaged: The Myth of Trans Identity as a Trend
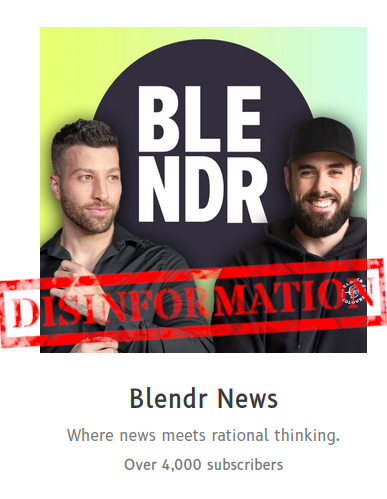
Another pernicious myth propagated by the article is the idea that the growing numbers of transgender youth, particularly trans boys, are really just lesbian and gay kids who are being "converted" by a social contagion. DeBoer claims that "65% of their referrals by 2019 were adolescent girls, many of whom had experienced sudden-onset dysphoria during puberty," and proceeds to list other attributes and attempts to correlate being trans with being autistic. The implication is that these youth are not "really" transgender but simply gender non-conforming, same-sex attracted, potentially autistic teens being misdiagnosed.
There are several problems with this claim. First, it relies on the false assumption that being transgender is a new "trend" corrupting youth, when in reality evidence shows that gender identity is a deeply innate trait, not something imposed by external influences. This is straight out of the Littman ROGD debunked nonsense playbook. DeBoer strongly suggests a reference to the concept of ROGD. This term has been used in discussions about cases where individuals, particularly girls, develop gender dysphoria seemingly abruptly, often coinciding with social or environmental factors rather than a lifelong experience of gender dysphoria.
Second, it ignores the fact that transgender identity and sexual orientation are distinct concepts - being trans does not negate also being gay, lesbian or bisexual. Studies show that a significant portion of transgender youth do identify as gay, lesbian or bisexual in terms of their sexual orientation.10 Acknowledging this overlap is not evidence of "conversion" but simply a reflection of the diversity within the LGBTQ+ community.11
It's true that many transgender youth, especially trans boys, may appear gender non-conforming or experience same-sex attraction prior to coming out as trans. However, this does not mean their gender identity is caused by their sexual orientation or that they are being "turned trans" by social influence. The far more likely explanation is that in a society still rife with homophobia and transphobia, it can take time for youth to understand and express their identity. Many trans people first come out as gay or lesbian before realizing that their feelings extend beyond just sexual attraction. Suggesting that these youth are not "really" trans is not only insulting but ignores the very real distress they experience from gender dysphoria. Furthermore, as the concepts and understandings of what being transgender is about are more broadly accepted and shared, it should be no surprise that we see an increase in people who are feeling that it is safe and acceptable to divulge this personal truth.
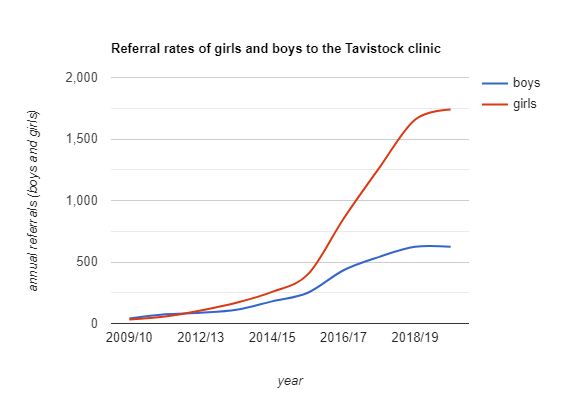
We have seen this historically as well, with a similar statistical plot-curve. When left-handedness became more socially accepted, the number of people identifying as left-handed increased significantly. This does not mean that there was a sudden rapid-onset left-handedness (ROLH) spreading socially across the country/world, or some other change leading to more left-handed individuals; rather, it reflects a change in social perception and acceptance. People who may have previously concealed their left-handedness due to stigma began to share openly that they are left-handed.
Notice how this plot-curve:
Seems similar to this one12:
For more on how this has been thoroughly and masterfully debunked, please check out Erin Reed’s13 article, as well as Julia Serano’s article14. ROGD is, in my opinion, more aptly named “Rapid Onset Parental Discovery.”
Detransition Deception: Putting Rare Experiences into Perspective
This brings us to the topic of detransition, which the article portrays as a common occurrence that is being ignored by the medical community. DeBoer claims that "less than a quarter of those who detransition even informed their clinicians" and that the most common reason is "realizing their dysphoria was related to other issues, not being transgender." The reality is that every reputable study to date has found that detransition is exceedingly rare, occurring in less than 1-3% of cases.15
Furthermore, research shows that the vast majority of those who do detransition do so due to external factors like family rejection, discrimination and difficulty accessing care, not because they realize they are not transgender.16 Detransition absolutely happens and those who experience it deserve support. However, it is incredibly rare, and fear mongering about it should not be used to argue against the importance of gender-affirming care for the vast majority of transgender youth who need it. As Serano rightly point out (links here are Serano’s as well):
Finally, it should stand to reason that based on the data we have explored, accepting trans people will reduce the number of detransitioners further.18
Beyond the Scare Stats: Mental Health Outcomes of Gender-Affirming Care
So what does the evidence actually say about mental health outcomes for transgender youth who receive gender-affirming care? Let's look at the facts. Every major medical organization, including the American Medical Association, American Academy of Pediatrics, American Psychological Association and Endocrine Society, has reviewed the research and concluded that gender-affirming care is medically necessary and potentially lifesaving for transgender youth. Their guidelines are based on a growing body of studies showing the positive mental health impacts of affirming care:
A 2020 Study in Pediatrics found that transgender adults who received puberty blockers as kids had significantly lower odds of lifetime suicidal ideation compared to those who wanted but did not receive this treatment. Specifically, the adjusted odds ratio for suicidal ideation in those who received puberty blockers was 0.3, indicating that they had 70% lower odds of experiencing suicidal ideation compared to those who did not receive the treatment.19
A 2014 study in Pediatrics found that gender-affirming hormone therapy was significantly associated with reduced depression and suicidality in transgender youth.20
A 2022 study in the The Journal of the American Medical Association found that transgender youth who received gender-affirming care had 60% lower odds of moderate or severe depression and 73% lower odds of suicidality compared to those who did not.21
In contrast, research has consistently shown the harms of denying transgender youth access to affirming care:
A 2024 Study from Nature and Human Behavior found that anti-transgender laws cause a significant increase in suicide attempts/ideation in trans youth of up to 72%.22
The 2015 U.S. Transgender Survey found that 40% of transgender adults reported attempting suicide in their lifetime, but those who had access to gender-affirming care had significantly lower rates.23
A 2021 study from The Trevor Project found that transgender youth who reported having at least one gender-affirming space had 25% reduced odds of attempting suicide in the past year.24
These are just a few examples of the many studies showing the potentially lifesaving impact of gender-affirming care.25 Of course, long-term outcome data is still limited given that comprehensive gender-affirming care for youth is a relatively recent development. More research is needed to optimize care. However, the evidence that does exist points strongly to the conclusion that gender-affirming care, when administered properly following established guidelines, can significantly improve mental health and reduce suicide risk in transgender youth.26
The Human Face of the Debate: Stories of Trans Youth and Families
What is often lost in the heated debates over gender-affirming care are the real life experiences of transgender youth and their families. It should come to no surprise that DeBoer does not interview or include personal stories of actual trans youth and their families. Underneath the rhetoric are countless stories of young people who were struggling with severe distress, depression and suicidality but found hope and healing through affirming care. There are youth like Alexa, who knew from a young age that their gender did not align with their body, leading to crippling anxiety and self-harm. With the support of gender-affirming counseling and medical care, Alexa was able to finally feel at home in their own skin and excel in school and relationships.27
Or like Alice, who as a child, would pray at night: “Can I please wake up as a girl? Can I please wake up as a girl?" she was transgender. After receiving gender-affirming care including hormones and surgery, Alice said "Finally, I feel like the person I was supposed to be – I feel like myself," These are not isolated cases but common experiences for transgender youth who are able to access the care they need.28
Equally important are the voices of transgender youth who might be denied access to gender-affirming care. Take Alabama for example, that recently has passed such legislation. "Why should some guy who has never met me ... why should he get to tell me what I can and can't do? Why does he get to decide what is right for people who just want to be happy?" asks Syrus, a trans man who knew he was a boy from a young age. When he started to go through female puberty, it started leading to depression. Syrus’ Mom says about him now: "He's more himself," Saunée says. "He's happy. You know, he's like a big kid. He'll still sit on my lap and cuddle up with me, and those are things he wasn't doing before." Syrus shares about his experiences: "I didn't have the words for what I felt" Syrus said. "I didn't fully have a grasp on gender until I found the words I needed." For Syrus, and many transgender people in Alabama, as NPR reports:
For Syrus, Alabama's legislation would deny something essential: the person he knows himself to be. And, he says, the notion that he's a "gender-confused child" who's just "going through a phase" causes real pain.
These stories put a human face on the very real costs of denying transgender youth access to care. They are not mere statistics but real people whose lives are impacted by the barriers placed in front of them. No one is claiming that gender-affirming care is a magic cure-all for every problem faced by transgender youth. Like any medical treatment, it has risks and benefits that must be carefully weighed. There is no one-size-fits-all approach, which is why the gender-affirming model emphasizes individualized care based on each youth's unique needs.30
Unfounded Funding Fears: Cashing In on Conspiracy Theories
The Blendr News article makes serious allegations about financial incentives and conflicts of interest driving the provision of gender-affirming care. While these claims deserve scrutiny, a closer look reveals a more complex picture that the article fails to acknowledge - moreover, it intentionally paints a misleading picture.
First and foremost, it is important to understand the distinction between revenue and profit. For the non-financial market wizards, revenue does not equal profit, and it's misleading for the article to conflate the two in suggesting financial motives were driving care at GIDS.
Revenue refers to the total income generated by an organization before accounting for any expenses. Profit is what's left over from the revenue after paying all the costs involved in operating and delivering services. So while the article makes a point of highlighting that GIDS accounted for 13.5-22% of the Tavistock Trust's income, that alone doesn't tell us anything about profitability.
Running a service like GIDS undoubtedly involves significant expenses - staffing, facilities, medications, etc. Without also reporting the costs and what percent of that revenue was actual profit, the article paints an incomplete and suggestive picture. Generating a lot of revenue for the Trust doesn't inherently mean GIDS was highly profitable or that financial incentives were driving treatment approaches.
The author seems to be relying on the implication that because GIDS brought in a lot of money overall, there must have been a profit motive pushing for medical intervention. So without providing the net profit numbers to support their claims, it becomes a big logical leap to make. It's entirely possible for something to generate a lot of revenue but have slim profit margins once expenses are accounted for.
With all that being said, it is true that by 2018/19, the Gender Identity Development Service (GIDS) accounted for a significant portion of the Tavistock and Portman NHS Foundation Trust's income. However, this figure reflects the increasing demand for and referrals to gender-affirming care, not an inherent profit motive. As a part of the UK's National Health Service, GIDS and the Tavistock Trust operate within a public healthcare system, not a for-profit model.
Moreover, providing comprehensive gender-affirming care, including extensive assessments, mental health support, puberty blockers, hormones, and surgeries, involves substantial costs. The cited revenue figures likely correspond to the real expenditures required to expand services to a larger population of transgender and gender-diverse youth. Without a detailed breakdown of costs and spending, the income percentage alone does not prove a conflict of interest.
The article also implies that pharmaceutical influence tainted the Dutch researchers' work on puberty blockers, noting their presentation at a conference sponsored by a maker of these drugs. However, it's crucial to recognize the strict ethical guidelines and disclosure requirements that govern medical research. The mere presence of industry sponsorship does not inherently undermine the integrity of the research, especially if that relationship is transparently disclosed. The focus should remain on evaluating the methodology and quality of the studies themselves.
It's important to reiterate that the gender-affirming care model, when properly administered, involves extensive assessments, counseling, and ongoing evaluation before any medical interventions are considered. This multidisciplinary approach, which is endorsed by major medical organizations, contradicts the notion that it's simply a reckless push for profit. The driving force behind the rise in youth seeking gender-affirming care is the growing awareness, reduced stigma, and recognition that it is a safe and valid path for those experiencing gender dysphoria - not a financial conspiracy.
Statistics show that the prevalence of transgender and gender-diverse youth has increased in recent years as acceptance grows. A 2022 study by the Williams Institute found that 1.4% of youth aged 13-17 in the US identify as transgender, up from 0.7% in 2017.31 In the UK, referrals to GIDS increased from under 100 in 2009/10 to over 2,500 in 2019/20.32 These numbers reflect the very real need for expanded services and support, not a manufactured trend for monetary gain.
While it's valid to consider potential conflicts of interest, the Blendr News article's claims of financial motives behind gender-affirming care paint a misleading and incomplete picture. By providing essential context and focusing on the evidence-based need for these services, we can refute the cynical notion that this globally recognized standard of care is reducible to a profit scheme. The well-being of transgender youth, not revenue, remains the driving force for the conscientious providers of gender-affirming care.
The Red Herring: The Irrelevant Infographic Scare Tactic
But what about that infographic that shows a growing market valuation?
No, I did not forget it, and here’s the thing folks - this is a red herring.
To make the implications of “transing the kids for profit” and “shady financial motives” stronger, they include a “Global Market Insights” infographic to show that the global market valuation is projected to grow, but instead of explaining that graphic or its (ir)relevance, it is never mentioned or referred to in the article. It serves only as a visual cue of some big numbers that look really damning when talking about these supposed “financial incentive” claims. As such, it needs to be addressed.
First and foremost, the data is completely irrelevant to the specific claims being made about the practices of the UK's Tavistock clinic and its GIDS program. Global market trends have no bearing on evaluating the quality of care at one particular clinic. It's a classic red herring fallacy, distracting from the core issues by introducing unrelated information.
Even worse, placing this graphic immediately after discussing the Tavistock Trust's revenue from GIDS heavily implies some connection between the clinic's practices and the growing sex reassignment surgery market. The article seems to be suggesting that the Tavistock was "cashing in" on this trend or had a profit motive to push kids toward surgery. However, absolutely no evidence is provided to support this serious accusation. It's a baseless insinuation made through misleading juxtaposition alone.
Additionally, the graphic's emphasis on the size of the male-to-female surgery market comes across as suggesting that vulnerable boys and men are being "transed" for financial gain by clinics like the Tavistock. This plays into the article's overall tone of conspiracy and fearmongering around youth transition care. But once again, no actual connection is drawn between this market data and the GIDS program, let alone any proof of financial incentives driving care decisions.
It's also critical to note that global surgery market projections tell us nothing about the prevalence of these procedures among youth, which is ostensibly the focus of this article. Including this data wrongly conflates trends across all age groups with the very specific context of adolescent transition care. It serves only to provoke alarm without illuminating any relevant evidence.
Perhaps most troubling is how DeBoer uses this graphic to weaponize information about a marginalized group to score ideological points. The provocative placement of these financial figures and growth rates seems calculated to make readers view the trans community with suspicion, as though their medical needs are some sort of "industry" rather than a matter of individual well-being. It's a tactic that dehumanizes trans people and breeds unwarranted hostility rather than understanding.
The use of this graphic is shockingly unethical. It relies entirely on innuendo and misdirection to compensate for the lack of any substantive evidence tying the Tavistock's practices to financial motives. Such blatant sensationalism has no place in journalistic coverage of a sensitive medical issue. The author should be ashamed to stoop to this level of baseless fearmongering and exposes its true nature as a work of propaganda rather than good-faith analysis.
Misinformation Kills: The Dangers of Stoking Fear for Clicks
However, spreading misinformation and stoking fear about gender-affirming care does nothing to help transgender youth and in fact puts them at greater risk. It is not a coincidence that 2021 and 2022 saw record numbers of anti-transgender bills introduced in state legislatures across the country, many of them seeking to ban or criminalize gender-affirming care for minors. These bills, based on the same sort of distortions and falsehoods promoted in the Blendr News article and others, have had devastating impacts on transgender youth and their families, driving some to uproot their lives and flee their home states in search of access to care.3334 Is it any wonder that 2021 was one of the deadliest years for trans people?35 One can draw a direct line between the amount of rhetoric targeting a minority and violence against said minority.363738
Others have not been so lucky. In 2022, at least one transgender youth attempted suicide in the weeks after Texas Governor Greg Abbott issued a directive ordering state agencies to investigate gender-affirming care as "child abuse."39 Their deaths were a tragic reminder of the very real harm caused by denying transgender youth access to medically necessary care and subjecting them to stigma and discrimination. We know that when politicians try to enact anti-trans laws, particularly targeting trans kids, the suicide rate increases.4041
It is clear that the misleading claims about gender-affirming care promoted by this article and other anti-transgender sources are not only factually inaccurate but actively dangerous. They contribute to a climate of fear, misinformation and discrimination that puts some of our most vulnerable youth at risk. As any LGBTQIA+ person, or parent of one will tell you, scare stories about trans youth are not an abstract issue for the community. They have a body count.
A Call to Do Better: Rejecting Junk Science and Protecting Trans Youth
Drawing this to a close, the accusations leveled against gender-affirming care in the Blendr News article are serious but ultimately without merit. A closer examination reveals a pattern of misrepresentation, cherry-picked anecdotes and disregard for scientific evidence. The reality is that gender-affirming care for transgender youth, when administered properly following established guidelines, is safe, effective and often lifesaving. It is not child abuse but medically necessary care supported by every major medical organization.
There is certainly room for robust discussion and research into how to optimize care and support for transgender youth. No one is claiming that the current system of gender-affirming care is perfect or that there are no valid concerns to address. However, those conversations must be rooted in facts and evidence, not sensationalized fear mongering. Spreading misinformation and stoking moral panic about "rushing" youth into transition or subjecting them to "chemical castration" does nothing to help transgender youth. As a matter of fact, it contributes to a climate of stigma and discrimination that puts their health and lives at risk. A better slogan for DeBoer and Blendr “News” might be:
Blendr News: Where Ideology Meets Misinformation
As a society, we must do better. We must reject the sort of biased, factually inaccurate reporting exhibited in this article and demand that journalism on this sensitive issue be rooted in science, not ideology. We must listen to the voices of transgender youth themselves and center their experiences and needs. And we must recognize that supporting access to gender-affirming care is not about politics but about protecting the health and well-being of a vulnerable population. As I have written elsewhere, supporting transgender youth is about love, not politics.42
Every young person deserves to feel safe, valued and respected for who they are. For transgender youth, that often means access to gender-affirming care to alleviate the distress of gender dysphoria and provide them the opportunity to thrive. Denying them that care based on myths and misconceptions is not only cruel but dangerous. As a society, we have a moral obligation to do better. The lives of transgender youth in your community depend on it.
Reed, Erin. (2024). Fact check: New York Times publishes misleading story on puberty blocker study. Retrieved from https://www.erininthemorning.com/p/fact-check-new-york-times-publishes ↩
Ibid. ↩
Rew, L., Young, C. C., Monge, M., & Bogucka, R. (2021). Review: Puberty blockers for transgender and gender diverse youth-a critical review of the literature. Child and adolescent mental health, 26(1), 3–14. https://doi.org/10.1111/camh.12437 ↩
Salas-Humara, C., Sequeira, G. M., Rossi, W., & Dhar, C. P. (2019). Gender affirming medical care of transgender youth. Current problems in pediatric and adolescent health care, 49(9), 100683. https://doi.org/10.1016/j.cppeds.2019.100683
https://pmc.ncbi.nlm.nih.gov/articles/PMC8496167/#:~:text=Treatment%20with%20gonadotropin,gender%20affirmation%20surgeries. ↩Janet Y Lee, Courtney Finlayson, Johanna Olson-Kennedy, Robert Garofalo, Yee-Ming Chan, David V Glidden, Stephen M Rosenthal, Low Bone Mineral Density in Early Pubertal Transgender/Gender Diverse Youth: Findings From the Trans Youth Care Study, Journal of the Endocrine Society, Volume 4, Issue 9, September 2020, bvaa065, https://doi.org/10.1210/jendso/bvaa065 ↩
Maria Anna Theodora Catharina van der Loos, Lidewij Sophia Boogers, Daniel Tatting Klink, Martin den Heijer, Chantal Maria Wiepjes, Sabine Elisabeth Hannema, The natural course of bone mineral density in transgender youth before medical treatment; a cross sectional study, European Journal of Endocrinology, Volume 191, Issue 4, October 2024, Pages 426–432, https://doi.org/10.1093/ejendo/lvae126 ↩
World Professional Association for Transgender Health. (2022). Standards of Care for the Health of Transgender and Gender Diverse People, Version 8. Retrieved from https://www.wpath.org/media/cms/Documents/SOC%20v8/SOC-8%20FAQs%20-%20WEBSITE2.pdf ↩
Wylie C Hembree, Peggy T Cohen-Kettenis, Louis Gooren, Sabine E Hannema, Walter J Meyer, M Hassan Murad, Stephen M Rosenthal, Joshua D Safer, Vin Tangpricha, Guy G T’Sjoen, Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society Clinical Practice Guideline, The Journal of Clinical Endocrinology & Metabolism, Volume 102, Issue 11, 1 November 2017, Pages 3869–3903, https://doi.org/10.1210/jc.2017-01658 ↩
American Academy of Pediatrics. (2023). Supporting Our Transgender and Gender-diverse Youth. Retrieved from https://www.aap.org/en/news-room/aap-voices/supporting-our-transgender-and-gender-diverse-youth/ ↩
Szoko, N., Sequeira, G. M., Coulter, R. W. S., Kobey, J., Ridenour, E., Burnett, O., & Kidd, K. M. (2023). Sexual Orientation Among Gender Diverse Youth. The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 72(1), 153–155. https://doi.org/10.1016/j.jadohealth.2022.08.016 ↩
Human Rights Campaign. (n.d.). Transgender children & youth: Understanding the basics. Retrieved from https://www.hrc.org/resources/transgender-children-and-youth-understanding-the-basics ↩
I am aware this is a flawed comparison, the point is not to be taken as a serious means to prove or disprove on this basis alone. The point is that we see a similar rapid increase over a short period of time once the perception surrounding a thing is no longer so socially taboo. ↩
Erin in the Morning. (n.d.). No evidence being transgender is a mental disorder. Retrieved November 20, 2024, from https://www.erininthemorning.com/p/no-evidence-being-transgender-is?utm_source=publication-search ↩
Serano, J. (2020, December 9). Everything you need to know about rapid onset gender dysphoria. Medium. Retrieved November 20, 2024, from https://juliaserano.medium.com/everything-you-need-to-know-about-rapid-onset-gender-dysphoria-1940b8afdeba ↩
Serano, J. (2021, February 1). Spotting anti-trans media bias on detransition. Medium. Retrieved November 20, 2024, from https://juliaserano.medium.com/spotting-anti-trans-media-bias-on-detransition-a9a782a46894 ↩
James, Sandy E.; Herman, Jody L.; Rankin, Susan; Keisling, Mara; Mottet, Lisa; Anafi, Ma'ayan (2016). "De-Transitioning" (PDF). The Report of the 2015 U.S. Transgender Survey (Report). Washington, DC: National Center for Transgender Equality. Archived (PDF) from the original on January 21, 2018. Retrieved March 18, 2019. ↩
Serano, J. (2021, February 1) - See 15 Above. ↩
GenderGP. (n.d.). Detransition facts. Retrieved November 20, 2024, from https://www.gendergp.com/detransition-facts/ ↩
Turban, J. L., Keuroghlian, A. S., & McGowan, K. (2020). Pubertal suppression for transgender youth and risk of suicidal ideation. Pediatrics, 145(2), e20191725. https://doi.org/10.1542/peds.2019-1725 ↩
Annelou L.C. de Vries, Jenifer K. McGuire, Thomas D. Steensma, Eva C.F. Wagenaar, Theo A.H. Doreleijers, Peggy T. Cohen-Kettenis; Young Adult Psychological Outcome After Puberty Suppression and Gender Reassignment. Pediatrics October 2014; 134 (4): 696–704. 10.1542/peds.2013-2958 Link: https://publications.aap.org/pediatrics/article-abstract/134/4/696/32932/Young-Adult-Psychological-Outcome-After-Puberty?redirectedFrom=fulltext ↩
Tordoff, D. M., Wanta, J. W., Collin, A., Stepney, C., Inwards-Breland, D. J., & Ahrens, K. (2022). Mental Health Outcomes in Transgender and Nonbinary Youths Receiving Gender-Affirming Care. JAMA network open, 5(2), e220978. https://doi.org/10.1001/jamanetworkopen.2022.0978 ↩
Lee, W.Y., Hobbs, J.N., Hobaica, S. et al. State-level anti-transgender laws increase past-year suicide attempts among transgender and non-binary young people in the USA. Nat Hum Behav 8, 2096–2106 (2024). https://doi.org/10.1038/s41562-024-01979-5 ↩
James, S. E., Herman, J. L., Rankin, S., Keisling, M., Mottet, L., & Anafi, M. (2016). The report of the 2015 U.S. Transgender Survey. National Center for Transgender Equality.
https://web.archive.org/web/20180121184448/https://transequality.org/sites/default/files/docs/usts/USTS-Full-Report-Dec17.pdf ↩The Trevor Project. (2021). National survey on LGBTQ youth mental health 2021. https://www.thetrevorproject.org/survey-2021/ ↩
GLAAD. (n.d.). Medical association statements supporting trans youth healthcare and against discriminatory legislation. Retrieved November 20, 2024, from https://glaad.org/medical-association-statements-supporting-trans-youth-healthcare-and-against-discriminatory/ ↩
Park, R. H., Liu, Y. T., Samuel, A., Gurganus, M., Gampper, T. J., Corbett, S. T., Shahane, A., & Stranix, J. T. (2022). Long-term Outcomes After Gender-Affirming Surgery: 40-Year Follow-up Study. Annals of plastic surgery, 89(4), 431–436. https://doi.org/10.1097/SAP.0000000000003233 ↩
ACLU of Indiana. (2021, June 21). Gender-affirming care saved my life. Everyone should have access to it. Retrieved November 20, 2024, from https://www.aclu-in.org/en/news/gender-affirming-care-saved-my-life-everyone-should-have-access-it ↩
UCLA Health. (2021, March 31). Gender affirmation services help patients live the lives they were seeking. Retrieved November 20, 2024, from https://www.uclahealth.org/news/article/gender-affirmation-services-help-patients-live-the-lives-they-were-seeking ↩
NPR. (2021, March 28). “It’s hurtful”: Trans youth speaks out as Alabama debates banning medical treatment. Retrieved November 20, 2024, from https://www.npr.org/2021/03/28/981225604/its-hurtful-trans-youth-speaks-out-as-alabama-debates-banning-medical-treatment ↩
World Professional Association for Transgender Health. (2022). Standards of care for the health of transgender and gender diverse people, version 8. Retrieved from https://www.tandfonline.com/doi/pdf/10.1080/26895269.2022.2100644 ↩
Herman, J. L., Flores, A. R., & O'Neill, K. K. (2022, June). How many adults and youth identify as transgender in the United States? The Williams Institute. https://williamsinstitute.law.ucla.edu/publications/trans-adults-united-states/ ↩
Dyer C. (2021). Gender dysphoria service rated inadequate after waiting list of 4600 raises concerns. BMJ (Clinical research ed.), 372, n205. https://doi.org/10.1136/bmj.n205
Link: https://www.bmj.com/content/372/bmj.n205 ↩PBS NewsHour. (2023, March 30). Texas ban on youth gender-affirming care pushes family to cross state line for treatment. Retrieved November 20, 2024, from https://www.pbs.org/newshour/show/texas-ban-on-youth-gender-affirming-care-pushes-family-to-cross-state-line-for-treatment#:~:text=It%20revokes,weaned%20off. ↩
ABC News. (2023, March 30). ‘Genocidal’: Transgender people begin to flee states with anti-LGBTQ laws. Retrieved November 20, 2024, from https://abcnews.go.com/US/genocidal-transgender-people-begin-flee-states-anti-lgbtq/story?id=99909913 ↩
Human Rights Campaign. (2021). Marking the deadliest year on record, Human Rights Campaign announces release of annual report on violence against transgender and gender non-conforming people. Retrieved from https://www.hrc.org/press-releases/marking-the-deadliest-year-on-record-human-rights-campaign-announces-release-of-annual-report-on-violence-against-transgender-and-gender-non-conforming-people ↩
Piazza, J. A. (2020). Politician hate speech and domestic terrorism. International Interactions, 46(3), 431–453. https://doi.org/10.1080/03050629.2020.1739033 ↩
Politico. (2018). Yes, political rhetoric can incite violence. Retrieved from https://www.politico.com/magazine/story/2018/10/30/yes-political-rhetoric-can-incite-violence-222019 ↩
The Conversation. (2020). When politicians use hate speech, political violence increases. Retrieved from https://theconversation.com/when-politicians-use-hate-speech-political-violence-increases-146640 ↩
NBC News. (2022, June 8). Trans child attempted suicide over Greg Abbott's 'child abuse' directive. Retrieved November 20, 2024, from https://www.thedailybeast.com/parents-of-trans-children-sue-texas-over-child-abuse-investigations-into-gender-affirming-care/ ↩
Lee, W.Y., Hobbs, J.N., Hobaica, S. et al. State-level anti-transgender laws increase past-year suicide attempts among transgender and non-binary young people in the USA. Nat Hum Behav 8, 2096–2106 (2024). https://doi.org/10.1038/s41562-024-01979-5
Link: https://rdcu.be/dVbdT ↩The Trevor Project. (2024). Anti-Transgender Laws Cause up to 72% Increase in Suicide Attempts Among Transgender and Nonbinary Youth, Study Shows. Retrieved from https://www.thetrevorproject.org/blog/anti-transgender-laws-cause-up-to-72-increase-in-suicide-attempts-among-transgender-and-nonbinary-youth-study-shows/ ↩
Pitt People. (2023, November 15). Supporting transgender youth is about more than just healthcare. Substack. Retrieved November 20, 2024, from https://pittpeople.substack.com/p/supporting-transgender-youth-is-about ↩